Objectives: Controversies have recently arisen regarding post-operative haemorrhagic complications in relation to the surgical procedures adopted for tonsillectomy. The authors set out to verify the relationship between surgical techniques and post-operative haemorrhage based on the analysis of data derived from multi-centric studies.
Materials and Methods: Multi-centric studies published between 2000 and 2015 were selected. The data relevant to haemorrhagic complications were elaborated by ANOVA test.
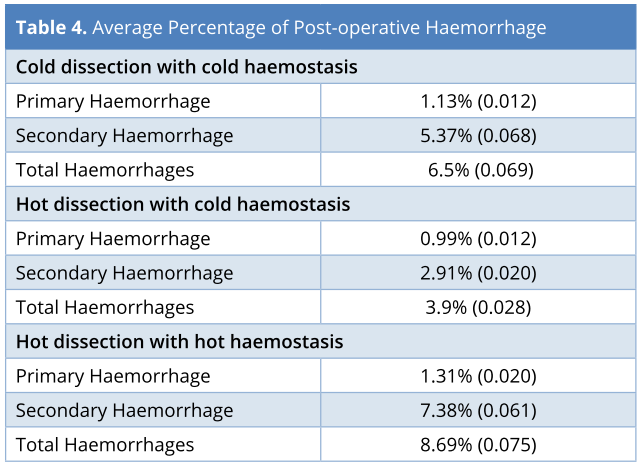
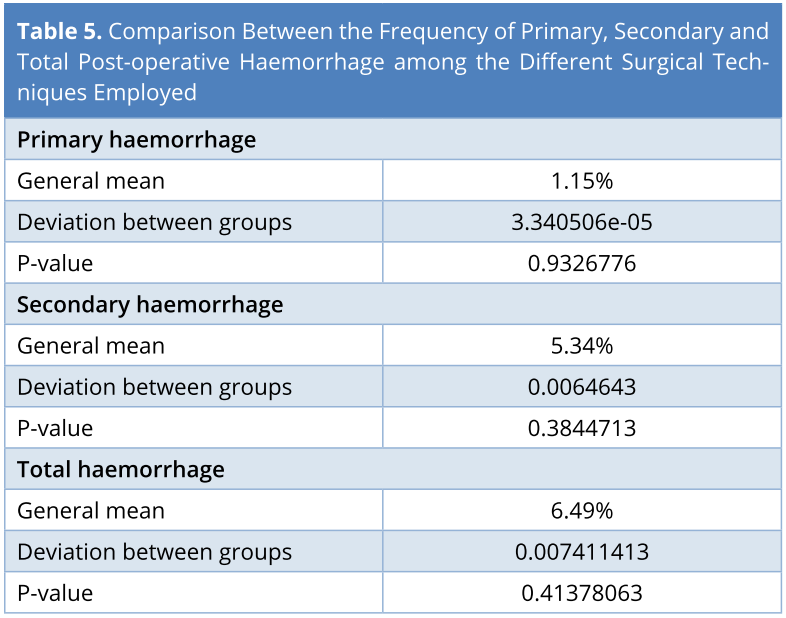
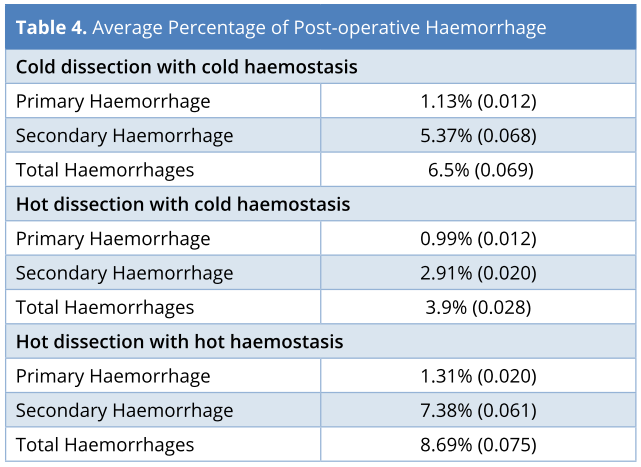
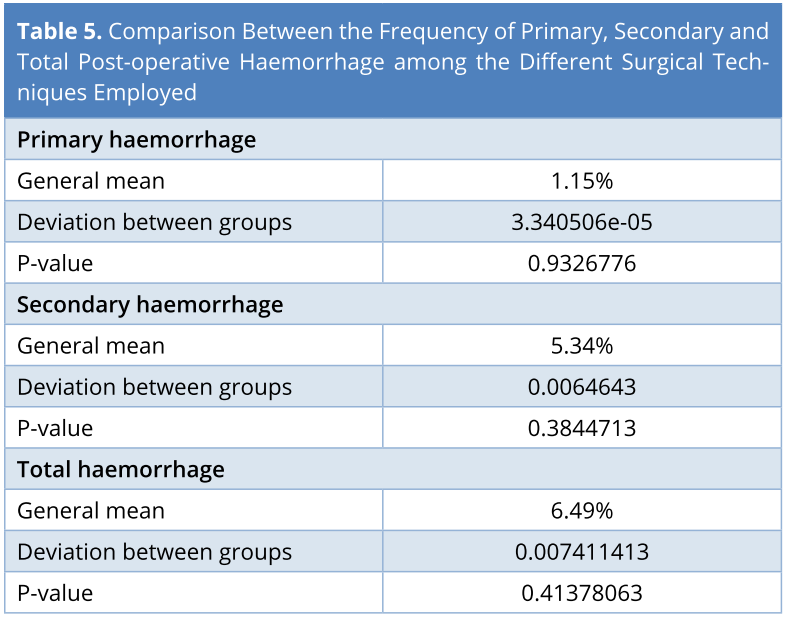
Results: Eight multi-centric studies were analysed. The mean frequency of post-tonsillectomy haemorrhage was: 1.13% for primary haemorrhage, 5.37% for secondary haemorrhage, and 6.5% as overall for cold dissection with cold haemostasis; 0.99% for primary haemorrhage, 2.91% for secondary haemorrhage, and 3.9% as overall for cold dissection with hot haemostasis; 1.31% for primary haemorrhage, 7.38% for secondary haemorrhage, and 8.69% as overall for hot dissection with hot haemostasis. The statistical comparison did not show significant differences between the frequencies of post-tonsillectomy primary, secondary, and total haemorrhage in relation to the surgical techniques employed.
Conclusion: A great variability in the frequency of haemorrhagic complications reported in the selected articles was found, regardless of the surgical technique. These findings, together with the lack of a statistically significant difference in post-tonsillectomy haemorrhage between the techniques employed, must be carefully considered by professionals involved in health organizations in clinical wards and the relative problems linked to medical liability.
Video Abstract
Adenotonsillar disease and the surgical treatments reveal that this condition may still raise concerns leading to the formulation of several guidelines [1,2], particularly in relation to potential post-operative complications [3]. Studies in literature present no uniform results regarding the general frequency of post-tonsillectomy haemorrhage [3] and the possible relationship between the type of surgical technique employed and the rate of haemorrhagic complications [4,5].
Post-tonsillectomy bleeding represents one of the most feared complications and constitutes an important cause of medical-legal dispute in otolaryngologic field [6]. Recent national guidelines on the appropriateness of tonsillectomy [7], as well as the studies specifically devoted to the safety of surgical techniques in tonsillectomy [8-12], give particularly rigid addresses that appear to be in contrast with some clinical research data [8,10,13,14] and that deserve a greater critical examination.
The present study has set out to verify the frequency of post-tonsillectomy haemorrhagic complications and the possible differences in post-tonsillectomy haemorrhage rate according to the most employed surgical techniques.
A MEDLINE inquiry was carried out using PubMed, Scopus, and Inter-Wiley as database, inserting the keywords “post-tonsillectomy haemorrhage” and “post-tonsillectomy bleeding”, and restricting the research to the studies published between 2000 and 2015.
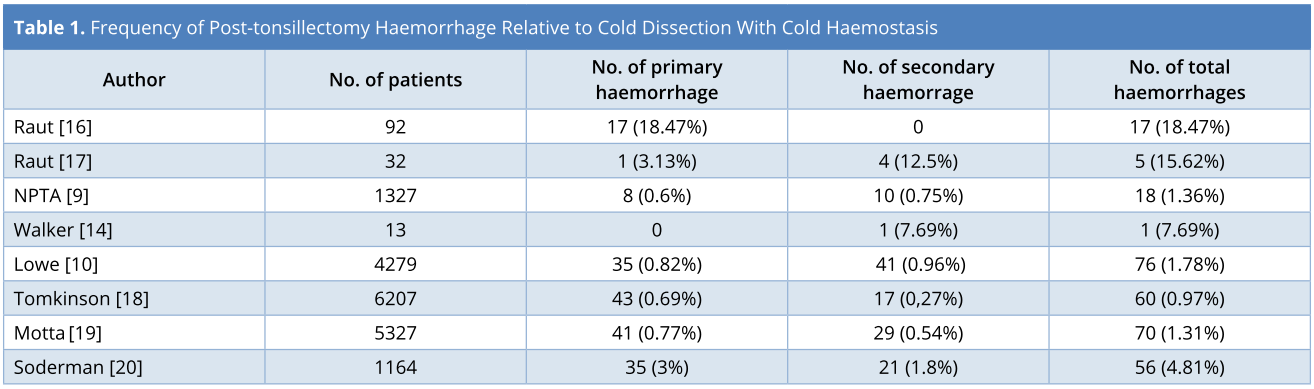
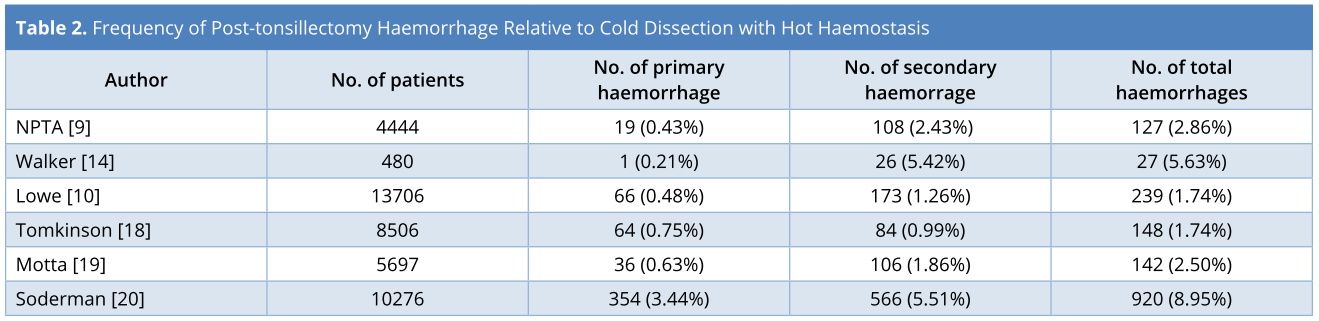
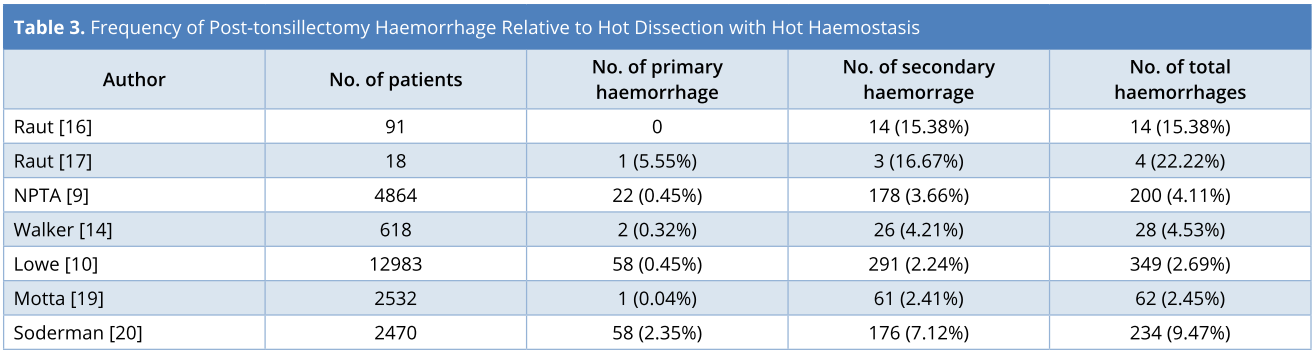
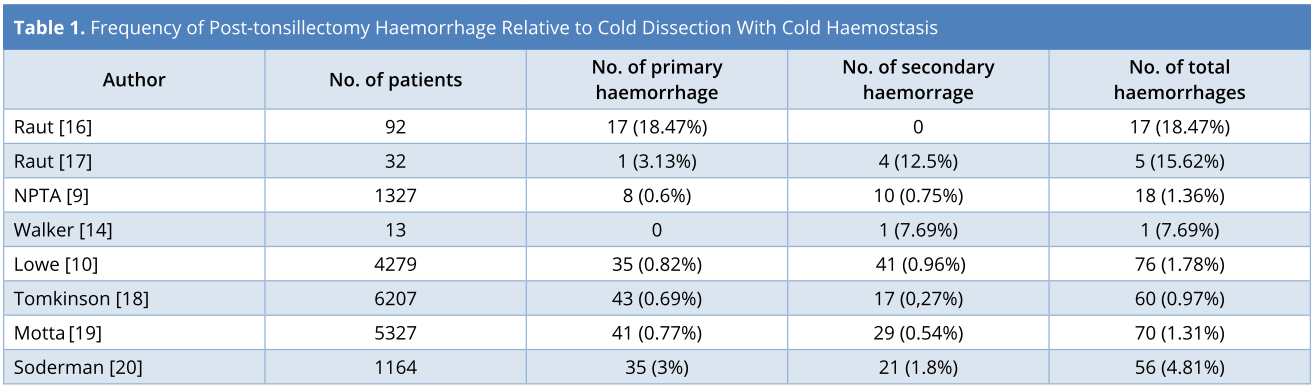
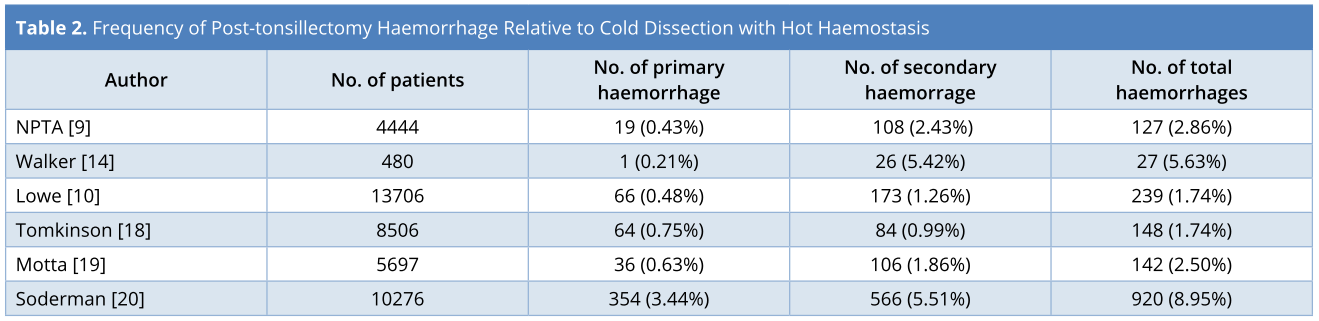
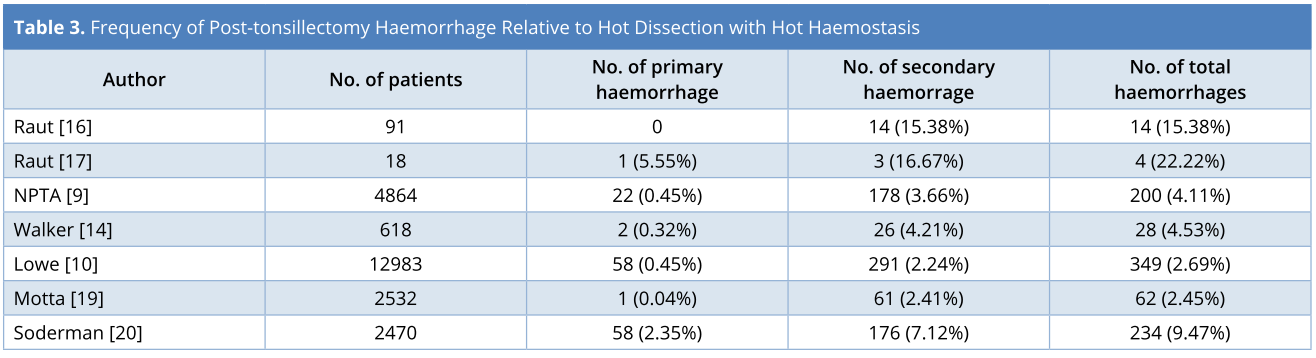
In total, 231 studies were identified. From these, the multi-centric English language papers were extrapolated, in which the three most commonly used dissection and haemostasis techniques [15] were analysed: cold dissection with cold haemostasis (CD/CH), in which the tonsillar dissection is achieved by the use of cold traditional instruments (scalpel, scissors, scaler) and the haemostasis is obtained by compression and ligature of blood vessels; cold dissection with hot haemostasis (CD/HH), in which the cold steel dissection is in combination with diathermy for haemostasis; hot dissection with hot haemostasis (HD/HH), in which the dissection and haemostasis are achieved by diathermy. The examined studies analysed such surgical techniques in relation to the percentage of post-surgical haemorrhage primary (occurring within the first 24 hours after surgery), secondary (occurring after 24 hours from surgery), and total, regardless of whether it had been necessary to return to the theatre to stop the bleeding.
Eight studies were selected, relative to the three techniques under examination (Tables 1-3), excluding a multi-centric study [21] in English language, as only the total percentage of post-operative bleeding was reported, and including a multi-centric Italian study conducted in 15 centres between 2002 and 2008 and published in 2011 [19].
In Lowe et al.’s [10] paper, the data divided by the authors into two groups - before and after the guidance issued by the National Institute for Clinical Excellence/British Association of Otolaryngologist, Head and Neck Surgeons in 2004 [22] — were analysed with reference to the global series.
ANOVA test was used to compare the surgical techniques under study, considering P < 0.05 as the minimum level of statistical significance. The data analysis was conducted using software R of the R Development Core Team, a free software distributed under the GNU GPL license.
The data, relative to the post-operative haemorrhage are reported in Table 4. No significant differences were found in the frequency of the primary, secondary and total haemorrhage among the different surgical techniques employed (Table 5).
Tonsillectomy is one of the most commonly performed surgical procedures [23, 24], although the scientific literature rarely provides the prevalence of tonsillectomy and adenotonsillectomy [25]. Some data are found for Denmark: approximately 7,000 annual tonsillectomies [26], Scotland: 14,530 (sum from 2002–2005) and 3,605 (sum from 2006–2007) [27], Sweden: about 10,000 procedures per year [28], England with Wales: 19,250 tonsillectomies per year [29], Italy: 44,000 (2000) [30], 59,916 (2002) and 51,983 (2003) [7], France: about 50,000 pediatric tonsillectomies each year [31], Great Britain: 78,000 (during 1994 and 1995) [32] and about 90,000 annual surgical procedures [33], and USA: 1,400,000 (1959), 500,000 (1979) [34], 286,000 (1994) [35,36] as well as 287,000 children (1996) [37] and 530,000 [38,39,1] and 250,000 annual pediatric tonsillectomy [40]. In Italy, the rate of tonsillectomy reported is of 10.7 (2000), 10.5 (2002), 9.1 (2003), and 9.4 (2004) per 10,000 inhabitants [41].
The continuing disagreement regarding the indication for tonsillectomy leads to different rates of this surgical procedure, both between nations [41,42] and within single countries [43].
The present study is focused on the three most commonly used techniques in tonsillectomy [44], namely, CD/CH, CD/HH and HD/HH.
Previous studies suggest that the different surgical techniques for tonsillectomy have different impacts on post-operative mortality [45], even though no technique has ever been described as the “gold standard” [46].
Hot techniques remain as the most widespread techniques in many countries [9]. Hot dissection is used in about 50% of tonsillectomies [20] in Great Britain, whereas in Australia 64% of tonsillectomies are performed using various types of “hot” techniques [47]. An investigation carried out in the USA in 2011 indicated the mono-polar cauterization as the most common technique for haemostasis in tonsillectomy [48]. In Sweden, the majority of procedures are carried out by hot techniques, whereas the cold techniques are seldom used nowadays [9].
Mowatt et al. [8] reported a significantly lower frequency of primary haemorrhage in the subjects who underwent hot technique or cold dissection with hot haemostasis, whereas the frequency of secondary haemorrhage was higher in the subjects who underwent cold technique surgery, although not significant (the data was significant only when coblation was used).
Lowe et al. [9], in the “Prospective National Audit” for the National Health Service, conducted a survey involving 277 hospitals and including data related to 33,921 patients. The authors found haemorrhagic episodes more frequently in the subjects operated by the “hot” techniques.
The reliability of these data, however, has been questioned by the authors themselves for the imprecise definition of primary or secondary haemorrhage (e.g. haemorrhage that has onset in the first 24 hours sometimes extends beyond this temporal limit) or for the partial information supplied by the responders. The authors also noted that the higher frequency of post-operative haemorrhage in subjects operated by cold technique, but in which hot haemostasis was carried out, could depend on the energy “dosage” employed.
Hilton [49] underlines the advantages that diathermy offers (reduced bleeding during surgery; shortening of surgical time), but also points out that the risks are practically negligible; in fact, its use brings about an actual increase in the number of bleeding episodes of only 1-2%.
However, haemorrhagic complications occur at very variable rates and are reported in the literature as between 0.3% and over 10% [41], independently of the surgical technique used; this could depend on a series of biases in the evaluation of the haemorrhagic event, amongst which we consider important to point out the following issues.
Definition of Bleeding and Chronology of Haemorrhagic Complications
Many authors report only those haemorrhages that required second surgery, whilst the others report all the episodes of post-tonsillectomy bleeding [5]; thus, in the publications in which only the haemorrhages that needed surgical treatment are considered, the rate of post-tonsillectomy haemorrhage is lower, but mortality percentages rise, compared to those studies in which all haemorrhages are reported [50].
In this regard, Tomkinson [18], not only reports the incidence of primary and secondary post-surgical haemorrhage, but also distinguishes slight haemorrhagic complications (primary and secondary) from those that required second surgery, thus giving a more precise evaluation of the true risk of post-operative bleeding associated with the surgical technique employed. In the same way Soderman [20] reports the percentages of post-operative bleeding, also specifying the percentage of patients that required second surgery.
The lack of information on the time interval between surgery and the onset of the haemorrhage renders the differentiation between the primary and secondary bleeding unreliable [51].
Definition of Surgical Technique and Role of the Surgeon
Some studies [52-54] indicate the cold technique as the “gold standard” for dissection, but the technique used to achieve haemostasis is not reported, and therefore it is impossible to establish whether the cold technique was used alone or a hot haemostasis was performed.
In the present study, only those scientific publications were selected, in which both the dissection and haemostasis techniques were specified, and the primary haemorrhage was distinguished from the secondary one with an accurate chronology of the haemorrhagic event.
The greater frequency of haemorrhage in those subjects in which hot haemostasis was performed could have been due to heat damage caused by diathermy coagulation of the vessels responsible for intra-operative bleeding [37,46]. However, cold dissection, just as any potential sutures for haemostasis, must be carried out with an extreme caution in order to avoid vascular damage, which could lead to successive bleeding [54-57].
It is probable, therefore, that the skill and experience of the single surgeon represents an important factor in the origin of these events. In the Italian multi-centric study of 2011, Motta et al. [19,52,58] did not find any statistically significant difference regarding the frequency of the primary, secondary and total haemorrhage, in relation to the surgical techniques employed.
On the other hand, the authors noted that the rate of haemorrhage reported by some of the medical institutions that took part in the study was significantly higher for the same techniques used. In light of these results, the authors conclude that this variability can be attributed to possible errors in the individual behavior of the surgeon himself, rather than the kind of technique adopted.
Age of Patient
Michael et al. [12] in a study on 337 cases (145 operated by cold technique, 192 by hot technique) observed a higher frequency of haemorrhage in the adults compared to the children, as confirmed by Mosges in a paper published in 2011 [59], according to which, the increased frequency of bleeding in adults could be due to variables independent of the surgical technique, such as the variability in compliance of patients with the post-operative instructions (post-surgical diet and physical rest), smoking, presence of comorbidity, conditions of the tonsils, and coagulation defects.
In this regard, Tomkinson et al. [18] underlined that in patients over 12 years of age, the risk of post-operative bleeding (primary or secondary) that required a surgical treatment was 1.5 to 3 times greater than the population of patients under 12 years of age.
This data is confirmed by Walker [14], who, in the evaluation of the frequency of post-tonsillectomy haemorrhage, observes how this increased in a statistically significant way above all for secondary haemorrhage in different groups of patients according to age, with a risk which ranges from 0.6% in the patients below 4 years of age to 10.1% in the patients over 18 years of age.
The present study does not demonstrate any significant difference in the primary, secondary and total haemorrhage frequency between the three surgical techniques studied, differently from other authors [8-12,24].
A considerably low frequency of haemorrhagic complications following tonsillectomy, with a notable difference between the studies, emerged from the publications examined. A wide variability in the rate of haemorrhage is generally verified, especially with regard to the hot techniques; this does not appear to be attributable to the technique employed, but to the other factors, amongst which, in our opinion, the most important are the experience of the surgeon and the modalities with which the diathermy of bleeding vessels is carried out.
These data and the results of similar and recent studies on this issue must be evaluated for the formulation of clinical recommendations regarding the choice of techniques to be used for tonsillectomy, and cause doubts on the value of the strict clinical recommendations regarding the choice of techniques to be used for tonsillectomy.
Received date: August 02, 2017
Accepted date: October 12, 2017
Published date: April 12, 2018
None
None
© 2018 The Author(s). This is an open-access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC-BY).
I have checked the revised article. It can be accepted for publication.
Article is fine. Please publish it.
 PDF
PDF