Disorders of mucociliary clearance (MCC) occur from thickening of the mucus so that cilia function is impaired. Or cilia may be impaired directly, as in Chlorine exposure. MCC disorders allow bacteria to remain in place and multiply. Since so many conditions are caused by failure of mucociliary clearance, it is of significant benefit to measure it and then use these measurements to guide therapy.
When you go to PubMed, there are only three articles on nasal cilia; 3,824 articles on mucociliary clearance; but 23,529 articles on sinusitis. After a quick review of the recent journal publications on sinusits, speaks of various therapies and treatments, I do not find articles of measuring the cilia or aiding mucociliary clearance (MCC).
Numerous studies have shown that when MCC is normal, the action of the cilia removes bacteria, dust and pollen from the respiratory system. Normally, sinuses are drained by mucociliary clearance [1].
Similarly, studies have shown that impairment of cilia function enables bacteria to remain in place, multiply, and cause infection. When MCC is deficient, pollen accumulates, with a sharp increase in numbers and concentration [2].
A clear example of the need to consider cilia function is that in cold air, cilia slow down. Patients who rush into the classroom in winter are more liable to catch a cold or a virus. When patients are taught to warm the nose by blowing into the warm hands first that may avoid the winter cold [3].
In empty nose syndrome, if the inferior turbinates are removed or damaged, often sinus infections are the result. The best therapy is to attempt to substitute for the missing cilia. Another example is the study that after sinus or nasal surgery, it may take many weeks for cilia function to return. One solution is to maintain antibiotic therapy. The other solution, to restore cilia function faster, is not regularly mentioned [4].
When we see a sinusitis patient after 3 weeks of antibiotic therapy, without evidence of improvement, measuring the MCC can be a best guide for further treatment. Today we have serious arguments to try to reduce antibiotic usage. By improving MCC, that would certainly help to reduce the use of antibiotics [5].
There are known toxic industrial products that impair cilia function. These include chromium, cadmium, nickel, and copper. Smog causes decreased cilia movement due to various combinations of O3, SO2, NO2, and NH3. These are characterized by frequent sinus infections. Stimulation of cilia function is beneficial in avoiding infections due to smog. Preservatives added to nasal solutions, such as benzalkonium, are known to impair cilia function [6]. The means of improving MCC need not be complicated. Even humming and green tea can be effective.
There are two distinct parts to MCC, namely the cilia and the mucous. Mucus is in two parts: the outer gel area and the inner sol layer that contains the cilia. Cilia move in synchrony in the inner sol layer. This movement moves the outer gel layer that contains goblet cells, mucin (glycoprotein), IgA, albumin, lactoferrin, and lysozyme. Between 1-2 liters of liquid are produced daily, hence there is a need for adequate daily intake of fluids [7].
Methylxanthines, such as aminophylline, theobromine, 3-isobutyl-1-methylxanthine (IBMX), and theophylline, enhance cilia beat frequency. Several popular nasal corticosteroid sprays such as Flonase® improve MCC.
Because of the value of IgA, lactoferrin and lysozyme in mucus, there needs to be a caution against excess irrigation. Lysozyme is an important part of natural defense against infection [12].
Humming at a low tone sounds like “oooommm” and resembles the long horns of the Australian Aborigines, the didgeridoo. It tends to vibrate both mucus layers and to restore ciliary movement. Humming for one minute hourly aids MCC problems [13]. Exercises such as trampolining Jumping and rope skipping can be used to stimulate MCC.
Epigallocatechin gallate (EGCG) in tea, is anti-inflammatory and is known to stimulate cilia movement. The theonine and catechins in green tea are anti-inflammatory products. A recent study reports that preparing the green tea via microwave brings out a higher percentage of these products [14].
Proteolytic enzymes such as papain from papaya and bromelain from pineapple thin the mucus and reduce inflammation. Clear Ease™ contains 500,000 units of bromelain and 1M units of papain. It is administered via buccal pouch to avoid stomach acid effect [15].
Chicken soup is an age-old remedy that has been shown to speed mucus flow. The book entitled “Sinus Relief Now” by Jordan S. Josephson devotes a chapter on how to make his grandmother’s effective chicken soup. It has been demonstrated that the chemicals from chicken soup have beneficial effects. Increased intake of fluids may thin the thickened mucus and aid cilia function.
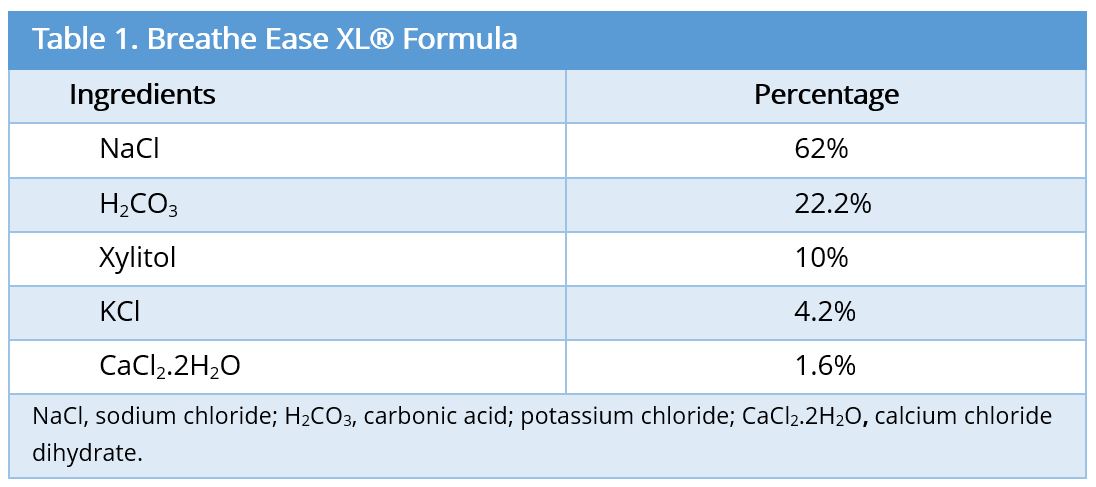
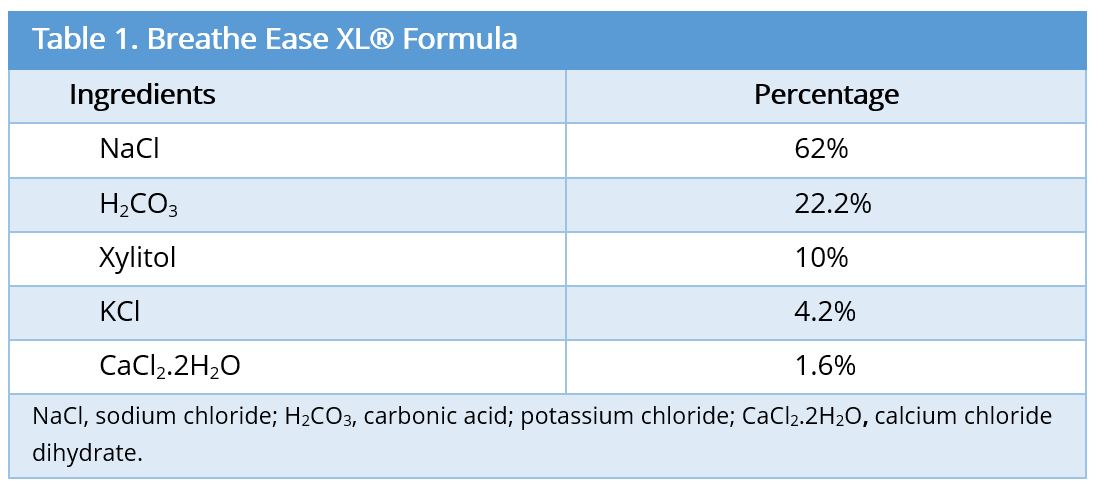
Caution is needed in use of irrigation fluids for sinus therapy. Boek has demonstrated that 0.9% saline may impair ciliary motion. Boek has shown that the Ringer’s formula is best for improving cilia function. Irrigating with prepared solutions that contain certain preservatives such as benzalkonium can impair cilia [16].
Various methods of measuring MCC include measuring the passage of isotopes through the upper respiratory system, and actually counting the cilia strokes. In the bronchi, bronchial MCC is measured using the radioaerosol technique [17].
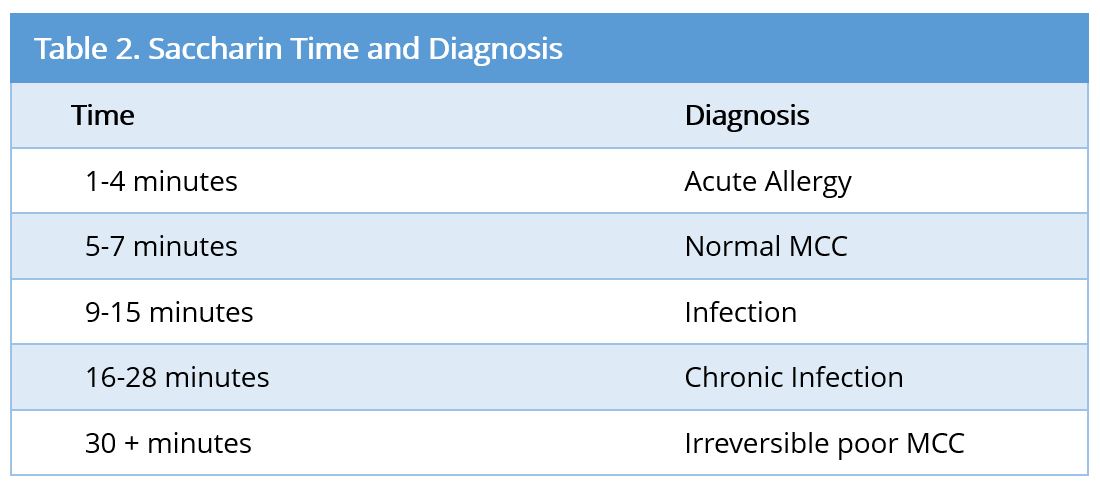
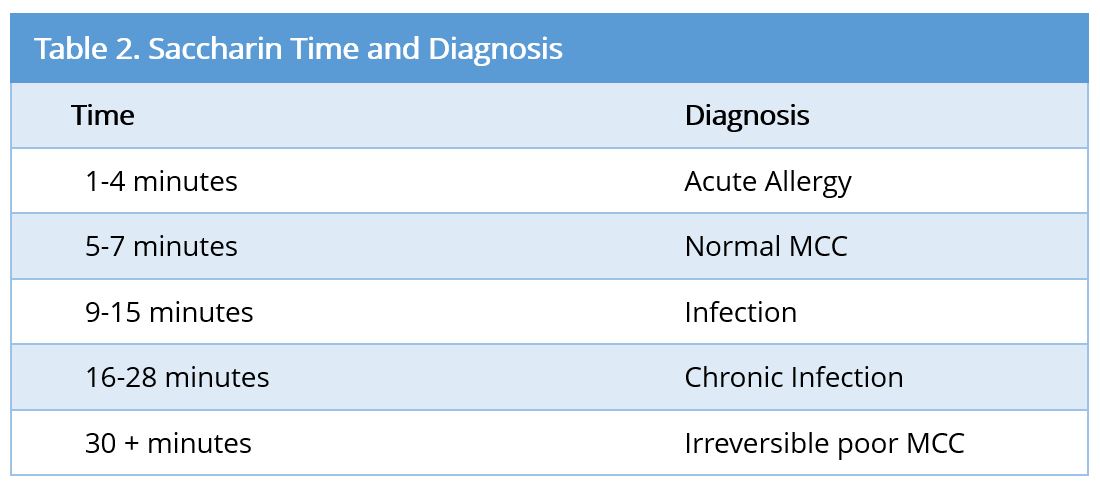
A clinical method of measuring nasal MCC is to place a particle of saccharin onto the medial surface of the inferior turbinate one cm back, and time how long it takes for the particle to reach the tongue where it is tasted. The saccharin test has established diagnostic standards (Table 2).
The Saccharin method is highly valuable for diagnosing toxic inhalants. Most important, it diagnoses why the patient is getting recurrent sinus infections and how to treat it [18].
Example 1: Jean M., age 25, called to be seen for acute sinusitis which she had at the same time last year. The saccharin test showed passage of saccharin in four minutes. Since this was the oak tree pollen season, the diagnosis of oak tree pollen allergy was easily made.
Example 2: I saw several patients form the airline industry, all of whom with poor MCC. It quickly developed that a new solvent they were inhaling was the cause, and the solvent was replaced [7]. Unfortunately, few industrial chemicals measure their effect on the MCC. Thus, the saccaha-rin test can indicate if a product impairs MCC. With the saccharin test, you can obtain an accurate figure of nasal function, and then repeat the test in order to get a valid finding of improvement or failure of certain thera-pies.
Many respiratory conditions can be classified as either having mucus too thick for normal ciliary beat frequency, or due to impaired cilia function as in chlorine gas inhalation. Fortunately, measuring the nasal cilia gives an accurate assessment of cilia speed in the bronchial tree as well as the nose. Best of all, measures to improve cilia of the upper respiratory system often work equally to aid cilia of the lower respiratory system as well. Increased attention to MCC will aid in the reduction of antibiotic abuse.
Received date: April 28, 2017
Accepted date: May 11, 2017
Published date: May 13, 2017
© 2017 The Author(s). This is an open-access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC-BY).
 PDF
PDF