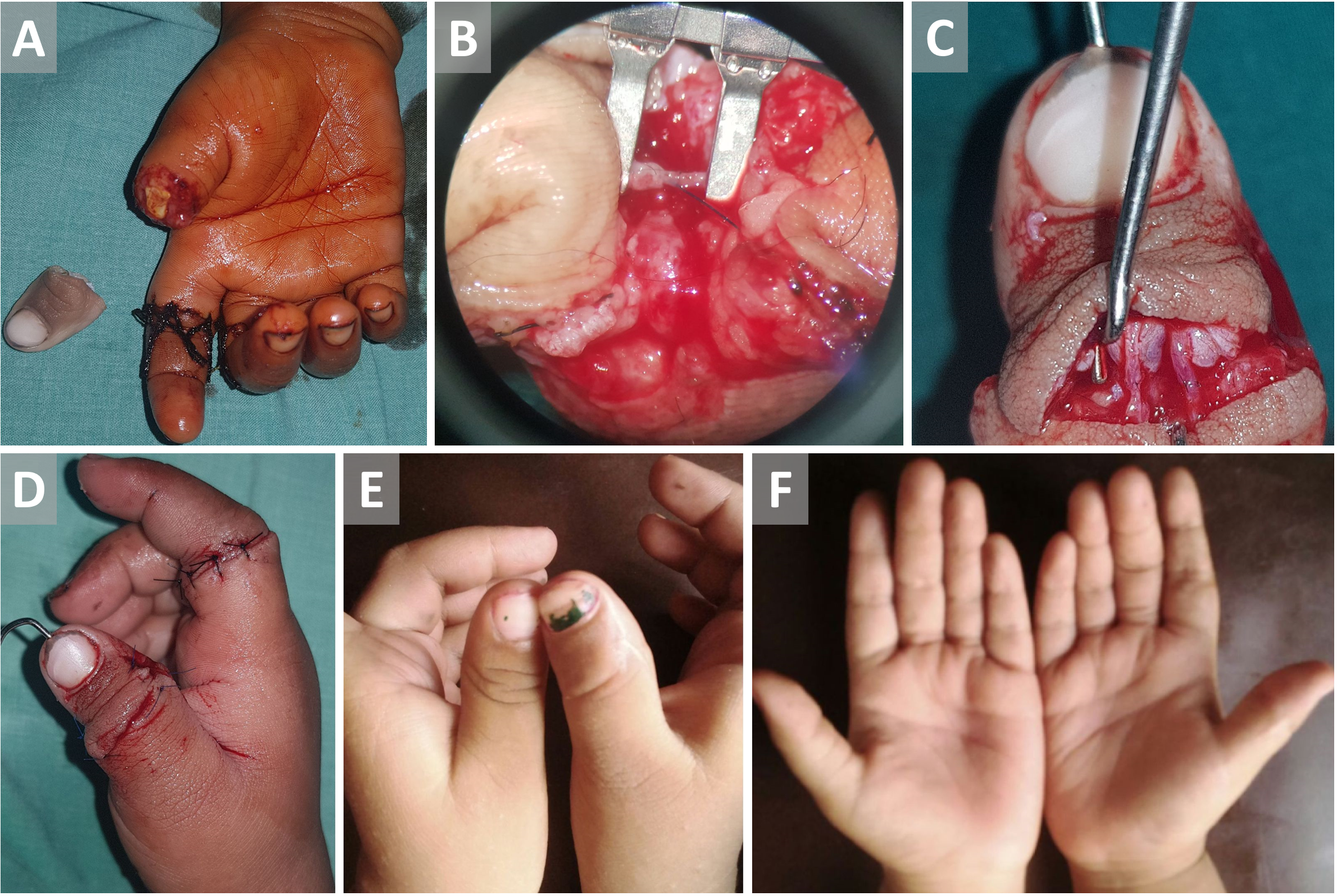
A 2-year-old child presented with total amputation of right thumb at the level of the interphalangeal joint (IPJ) after 6 hours of sustaining a machine cut injury. He also had a sutured laceration over the index finger. The distal and proximal amputated stumps were explored and neurovascular structures were tagged for replantation. Interphalangeal joint arthrodesis was performed with an axial K-wire. Radial digital artery on either side was chosen for arterial anastomosis. The vessel diameter was 0.5 mm. A 10 mm long intravascular stent (5-0 nylon) was prepared as described by Narushima M et al. [1]. The nylon stent was inserted into the amputated stump radial digital artery and 0-180 suture was conventionally performed with 11-0 nylon. A couple of stitches were applied over the back wall and the final two stitches over the anterior wall were tied after stent removal as described by Tashiro K et al. [2]. The anastomosis was completed in 20 minutes. Two dorsal veins were then anastomosed. Digital nerves were repaired. After six weeks, the K-wire was removed and the patient recovered well (Figure 1, video link: https://youtu.be/8nF9R9w2eLI).
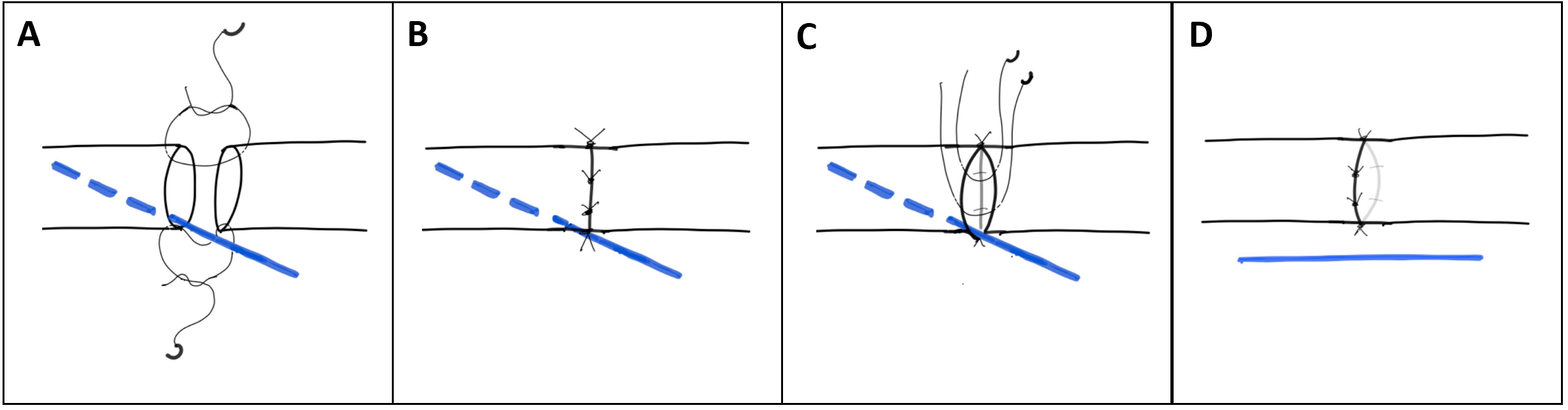
Hemi-intravascular stenting (hemi-IVaS) is used for super microsurgical anastomosis when one side of the vessel is damaged or thin [2]. In contrast to the classical intravascular stent anastomosis, in hemi-IVaS, only the stent is placed in one of the vessel lumen and vessel suturing is done manipulating the stent (Figure 2). It is also used in cases of vessel diameter discrepancy ≥1.5 times. These scenarios are usually encountered in the lymphovascular anastomosis, perforator to perforator anastomosis, and fingertip replantations. In our case, it was an amputation at the level of IPJ and there was no vessel diameter discrepancy. The performance of super microsurgical anastomosis with this technique was easier and faster. As the back wall was visible during anterior wall suturing, it was a secure way of anastomosing tiny vessels. To conclude, hemi-IVaS is a convenient technique which makes supermicrosurgical anastomosis simpler and easier.
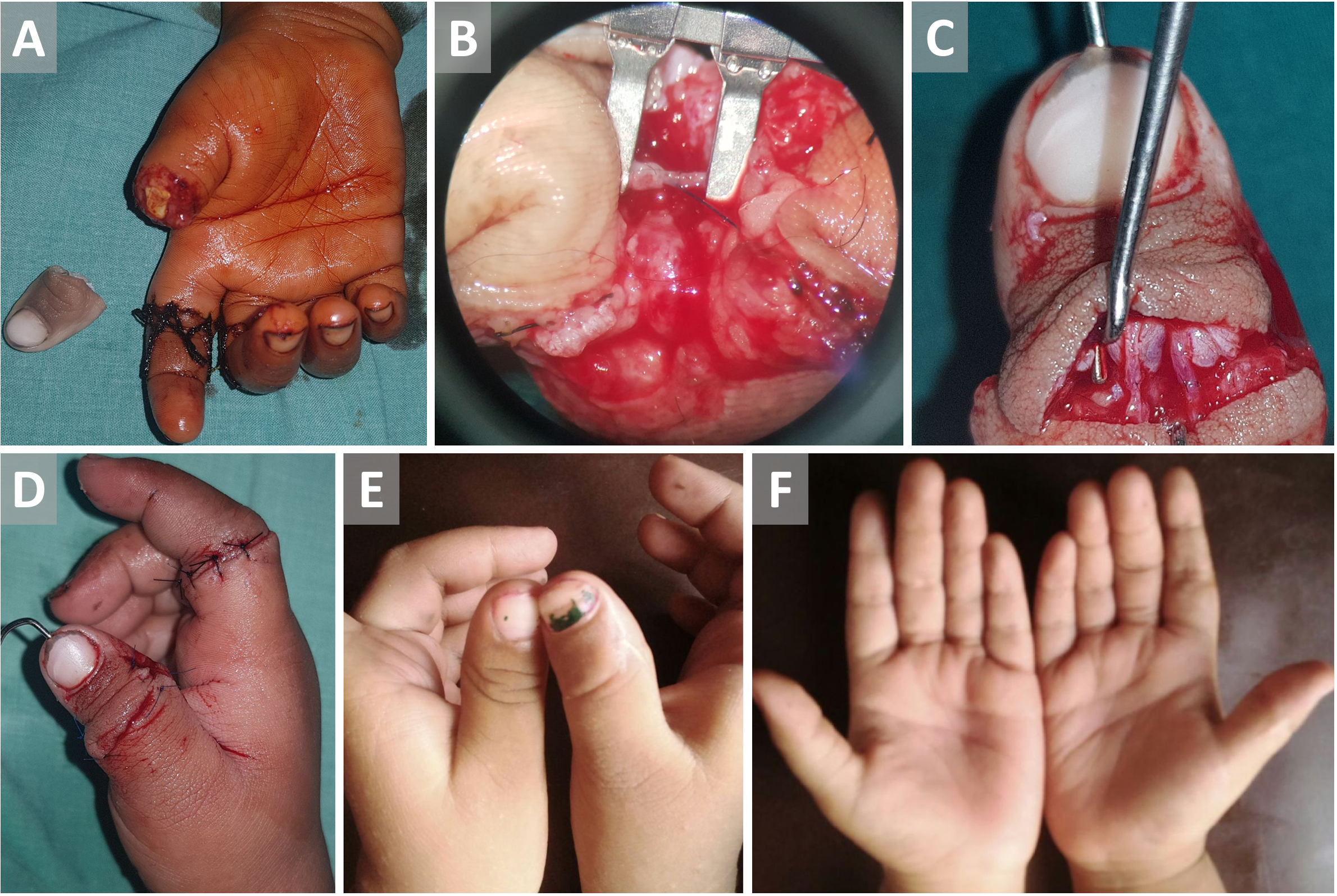
Figure 1. (A) Total amputation of right thumb & previously sutured ring finger laceration. (B) Arterial anastomosis with stent in situ. (C) Repaired dorsal digital veins. (D) Thumb after successful replantation. (E, F) Well-settled thumb dorsal and ventral views respectively.
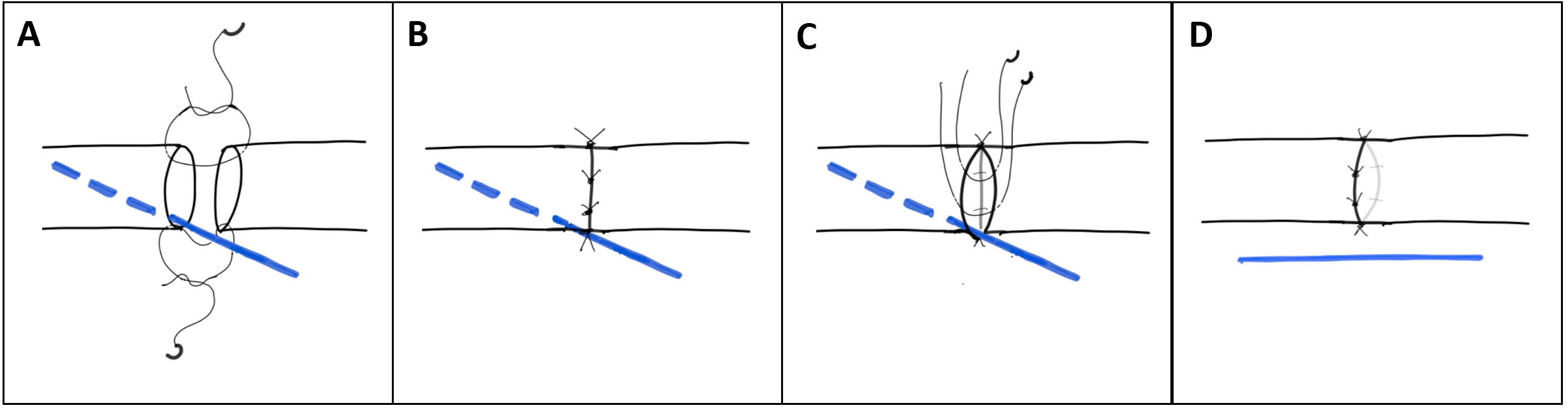
Figure 2. Hemi-intravascular stenting technique during arterial anastomosis. (A) Stent inside one of the anastomotic vessels during 0-180 suture (the blue line indicates the stent and the broken line indicates the intravascular portion of the stent). (B) Two stitches at the posterior wall after flipping the vessel. (C) Stent in situ and two untied stitches over the anterior wall. (D) Stitches are tied over the anterior wall after the stent removal.
Received date: March 27, 2019
Accepted date: May 14, 2019
Published date: June 12, 2019
The study is in accordance with the ethical standards of the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
The study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
The authors report no financial or other conflict of interest relevant to this article, which is the intellectual property of the authors.
© 2019 The Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC-BY).
Dave A, Saha S, Naalla R, Singhal M. Hemi-intravascular stenting technique for super microsurgical anastomosis in pediatric thumb replantation. Int Microsurg J 2019;3(2):3. https://doi.org/10.24983/scitemed.imj.2019.00114
 PDF
PDF