Introduction: Cognitive impairment and dementia constitute an important health problem in the geriatric population. Nowadays, the prevalence of these alterations has increased, especially as a result of progressively longer life expectancy. Different studies have shown the risk of hyperglycemia and hypoglycemia and its association with cognitive function in the population with diabetes. The objective of this study is to establish the physical dependence level and the cognitive impairment degree as well as its potential association with diabetes and hypoglycemia risk.
Methods: A multicenter cross-observational study was performed with the participation of 654 institutionalized residents of nursing homes to analyse anthropometric data, prevalence of diabetes, disability, and cognitive impairment associated with this metabolic disease.
Results: The average age of the sample was 82.4 years. The prevalence of diabetes amounted to 23.5%. Moreover, 7.8% of them remained with HbA1c > 8.5%, while 54.2% presented with HbA1c ≤ 6.5% with a high risk of hypoglycemia. The average disability of the global sample was moderate with an average of 43.8 points on the Barthel Index and the average of mistakes in the Pfeiffer test was 5.5, showing a mild cognitive impairment. We found a significant association between HbA1c less than 6% and higher cognitive impairment in diabetic cases (P = 0.04).
Conclusion: Diabetes control in the studied population could be too strict, and consequently, hypoglycemia in these patients could play a role in the major decline of cognitive function. Therefore, avoiding treatments that could lead to hypoglycemia in these patients could be very important. The aim of the treatment of diabetes in elderly patients is focused on stabilization, prevention of acute complications, and improving the quality of life.
Cognitive impairment and dementia constitute an important health problem in the geriatric population. Nowadays, the prevalence of these alterations has increased, especially as a result of progressively longer life expectancy [1]. In Spain, type 2 Diabetes Mellitus (T2DM) prevalence in the population aged over 65 years is between 10 to 15%, and more than 20% at 80 years [2]. Several studies indicate that the risk of cognitive impairment related to T2DM increases with age [3-5]. The brains of older people are especially vulnerable to hypoglycemia effects [6]. After every hypoglycemic episode, major cognitive changes could occur [7]. Diabetic patients do not usually obtain satisfactory results in neuro-psychological tests, which particularly involve attention and executive functions [8].
Objectives for glycated hemoglobin (HbA1c) in older adults should generally be 7.5% to 8%. However, an HbA1c level between 7% and 7.5% may be acceptable when healthy older adults without comorbidities and good functional status are included. Higher HbA1c levels (> 8.5%) are acceptable for older adults with multiple comorbidities and short life expectancy (usually less than one year) [9]. Moreover, there is potential harm in lowering HbA1c to less than 6.5% in older adults with T2DM [10,11]. One of the main characteristics of the geriatric population is their heterogeneity, presenting high comorbidities, changes in body composition, and an increased level of physical dependence and cognitive impairment; these factors often cause nutritional problems and a propensity to develop T2DM and its complications [12,13]. Due to these syndromes, the need of self-care and the probability of institutionalization increase. T2DM is one of the pathologies that require more care in these centers [14].
The objective of this study is to establish the physical dependence level and the cognitive impairment degree, as well as its potential association with T2DM and hypoglycemia risk related to a strict control of HbA1c levels required by this population group.
A multicenter cross-observational study was performed with the participation of 654 patients from six geriatric and gerontological care centers in Galicia (Spain), from October 2012 to March 2016. Nursing homes were selected by geographical location and volume of patients. All patients were informed in detail about the aims of the present study and its interventions, including the review of their clinical history, completion of complementary tests and scales. Informed consent was signed by every participant or legally authorized representative and the rights of the participants were protected throughout the study.
The following inclusion criteria were used: Volunteer participants living in nursing homes for more than six months before the commencement of the study signed an informed consent form in accordance with the informed consent law. In the case of patients with any grade of cognitive impairment, their legal guardians signed the informed consent form on their behalf. The exclusion criteria comprised the cases whose clinical history did not meet all the study variables, the patients who had been residing in the studied geriatric centers for less than six months at the time of commencement of the study, and the persons with guardianship in Foundations whose policies did not allow participation in studies.
For all patients the following information was obtained from their clinical history: age, sex, Body Mass Index (Kg/m2), Diabetes Mellitus diagnosis, diabetes treatment, and diagnosed macrovascular and microvascular complications. When patients were included in the study, a functional and cognitive geriatric assessment was made using the Pfeiffer test [15] (cognitive assessment) and the Barthel index [16] (functional assessment). A blood sample was also collected at that time to obtain HbA1c level.
Functional status was evaluated using the Barthel Index that measured the basic activities of daily living. This index assesses several physical dependence domains. Scores below 20 points identify total dependence, scores between 20 to 35 points show severe dependence, and scores between 40 to 55 and 60 to 95 points indicate moderate and mild dependence, respectively; 100 points identify that the patients are physically independent.
Cognitive status was evaluated using the Pfeiffer test. It is used as a screening tool that can help to detect cognitive impairment. It has sensitivity close to 70% and a very high specificity close to 95%. Scores higher than 8 mistakes identify severe cognitive impairment, and scores between 5 to 7 and 3 to 4 mistakes show moderate and mild cognitive impairment, respectively. Normal cognitive status is identified by 0 to 2 mistakes.
A descriptive analysis was used. Qualitative variables were obtained by means of proportions calculation. Quantitative variables were obtained by averages, standard deviation, and maximum and minimal ranges.
As a test of normality in continuous variables, Kolmogorov-Smirnov's test with Lillefors's correction and Shapiro-Wilk test were used. The normal variables were expressed as an average and standard deviation, and not Gaussian variables as a median and range. To compare variables Chi square test, Mann Whitney U test, and Kruskal-Wallis test were used.
The analyses were performed using SPSS V. 22 for Windows.
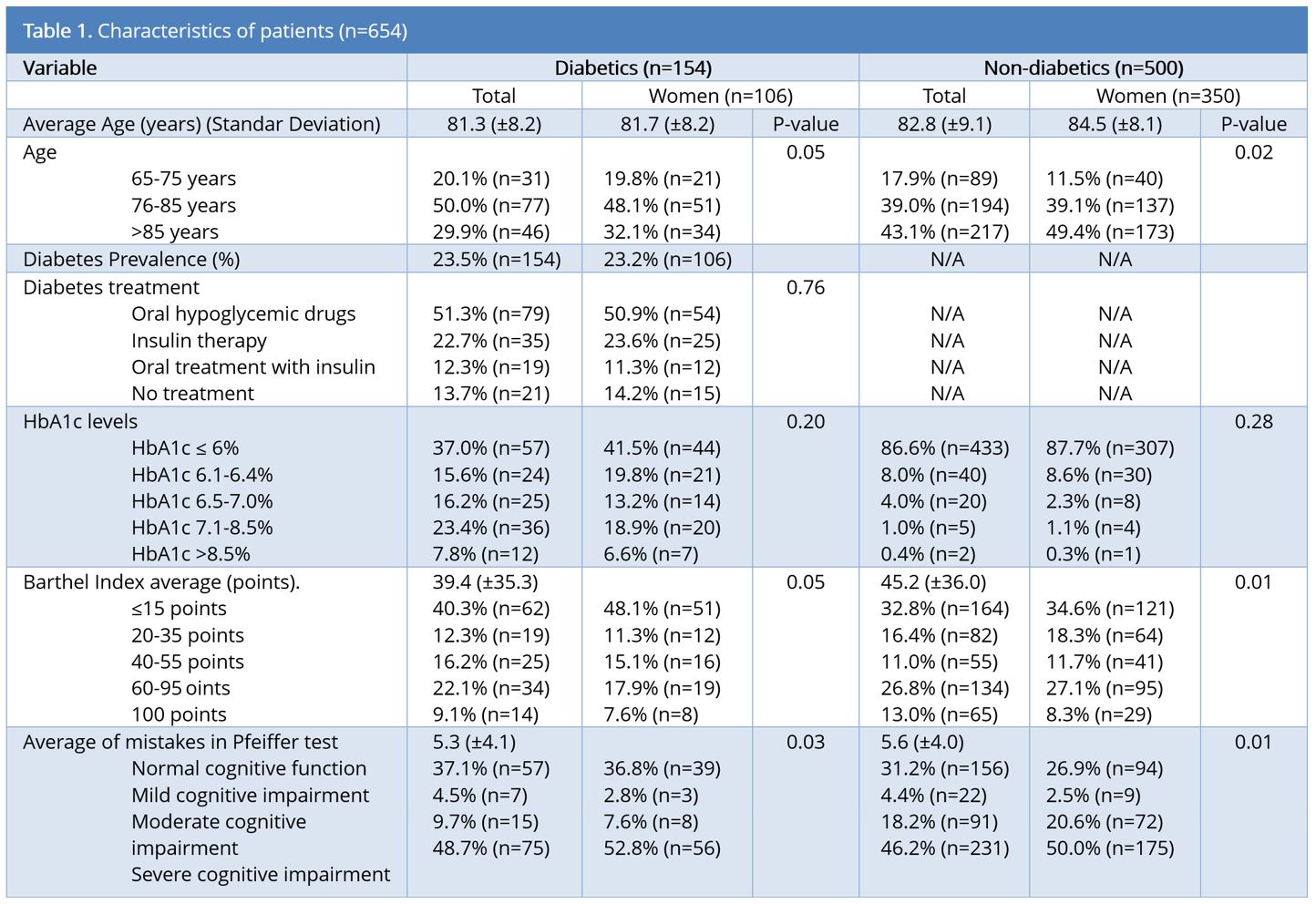
The number of residents in the selected centers was 925 potential candidates, of which, 654 cases fulfilled all inclusion criteria and none of the exclusion criteria. The average age of the sample was 82.4 (± 8.9) years. There was a predominance of women as they accounted for 69.7% (n = 455) of the sample (Table 1).
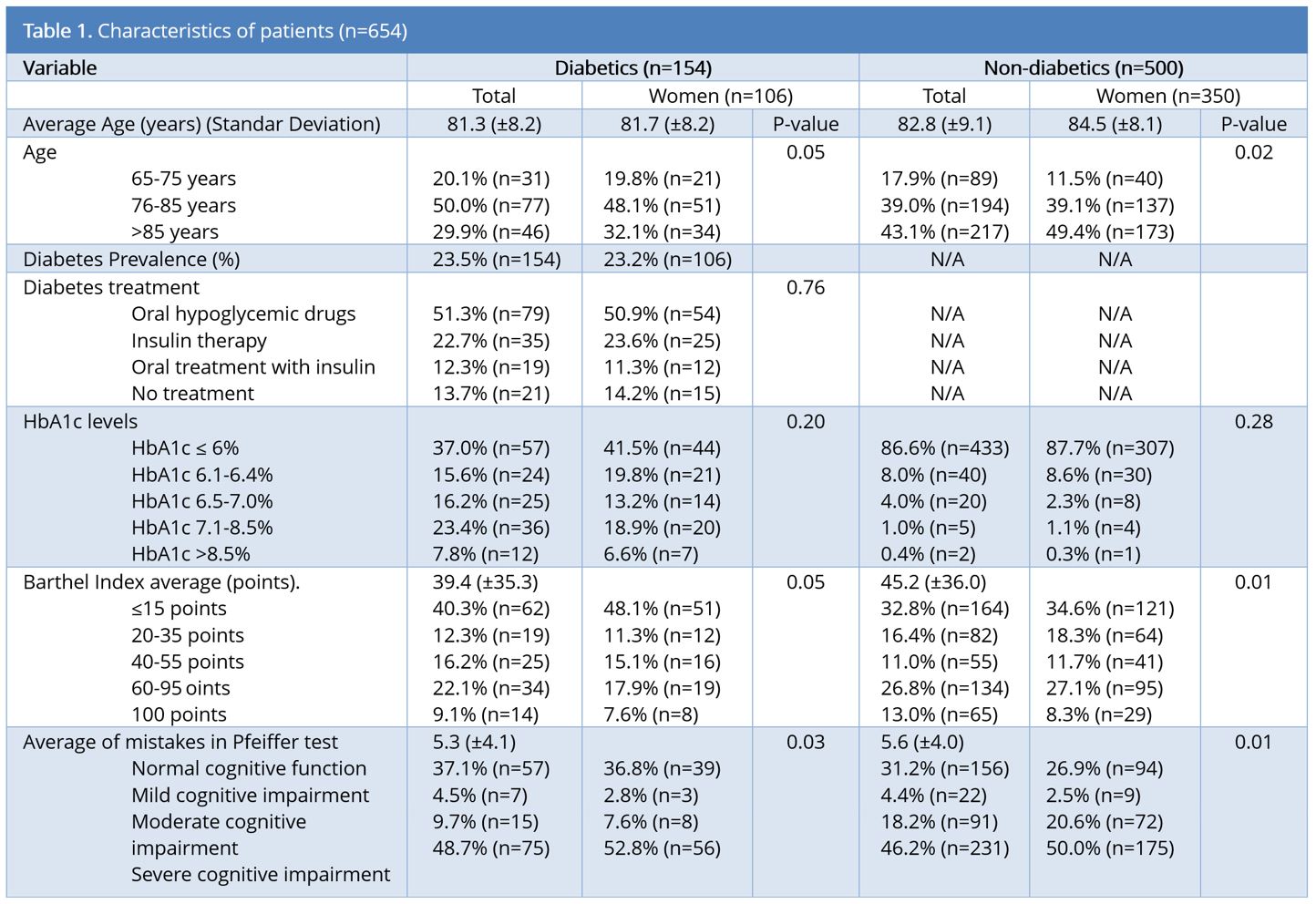
Diabetic cases had an average of 5.3 ± 4.1 mistakes in the Pfeiffer test. Non-diabetic cases had 5.6 ± 4.0 mistakes. Only 33% (n = 216) of the participants obtained a normal cognitive status. 47.2% (n = 305) had a severe cognitive impairment. By sexes, 73.8% (n = 225) were women, who had a higher cognitive impairment grade than men (P = 0.03).
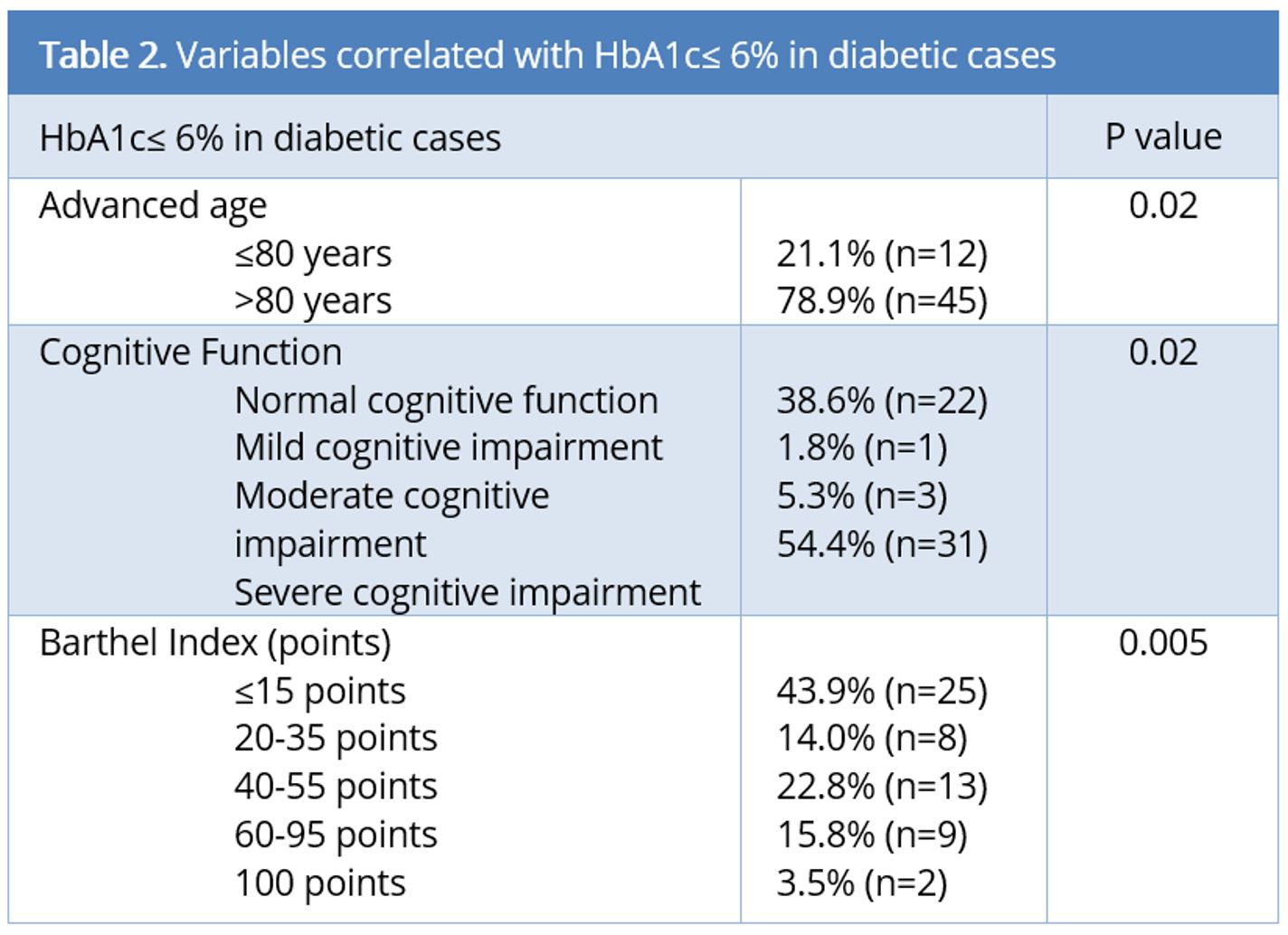
Cognitive status worsened with age. 52.8% (n = 47) of cases aged between 65 to 75 years and 67.1% (n = 153) between 86 to 95 years had moderate or severe cognitive impairment. Patients treated with insulin had a worse cognitive status (P = 0.02). 57.4% (n = 20) of diabetic patients treated with insulin had severe cognitive impairment. In our study, there was no association between oral antidiabetic drugs and cognitive impairment (p value > 0.05). 40.5% (n = 32) of diabetic patients treated with oral antidiabetic drugs had severe cognitive impairment. 54.4% (n = 31) of diabetic patients with HbA1c levels ≤ 6% had severe cognitive impairment. A significant association between HbA1c levels ≤ 6% and severe cognitive impairment (P = 0.04) in diabetics was observed, but no such association was found in non-diabetic patients. 38.6% (n = 22) of documented diabetic patients with levels of HbA1c ≤ 6% obtained a normal cognitive status in the Pfeiffer test. On the other hand, 54.4% (n = 31) had severe cognitive impairment and HbA1c levels compatible with high risk of hypoglycemia. In contrast, out of the total number of patients with moderate or severe cognitive impairment, only 6.6% (n = 7) of the cases presented with HbA1c levels above 8.5%. Non-diabetic cases with low HbA1c levels (under 6.5%) and severe cognitive impairment represent 46.4% (n = 217). We found no association between low HbA1c levels and cognitive impairment (P = 0.89).
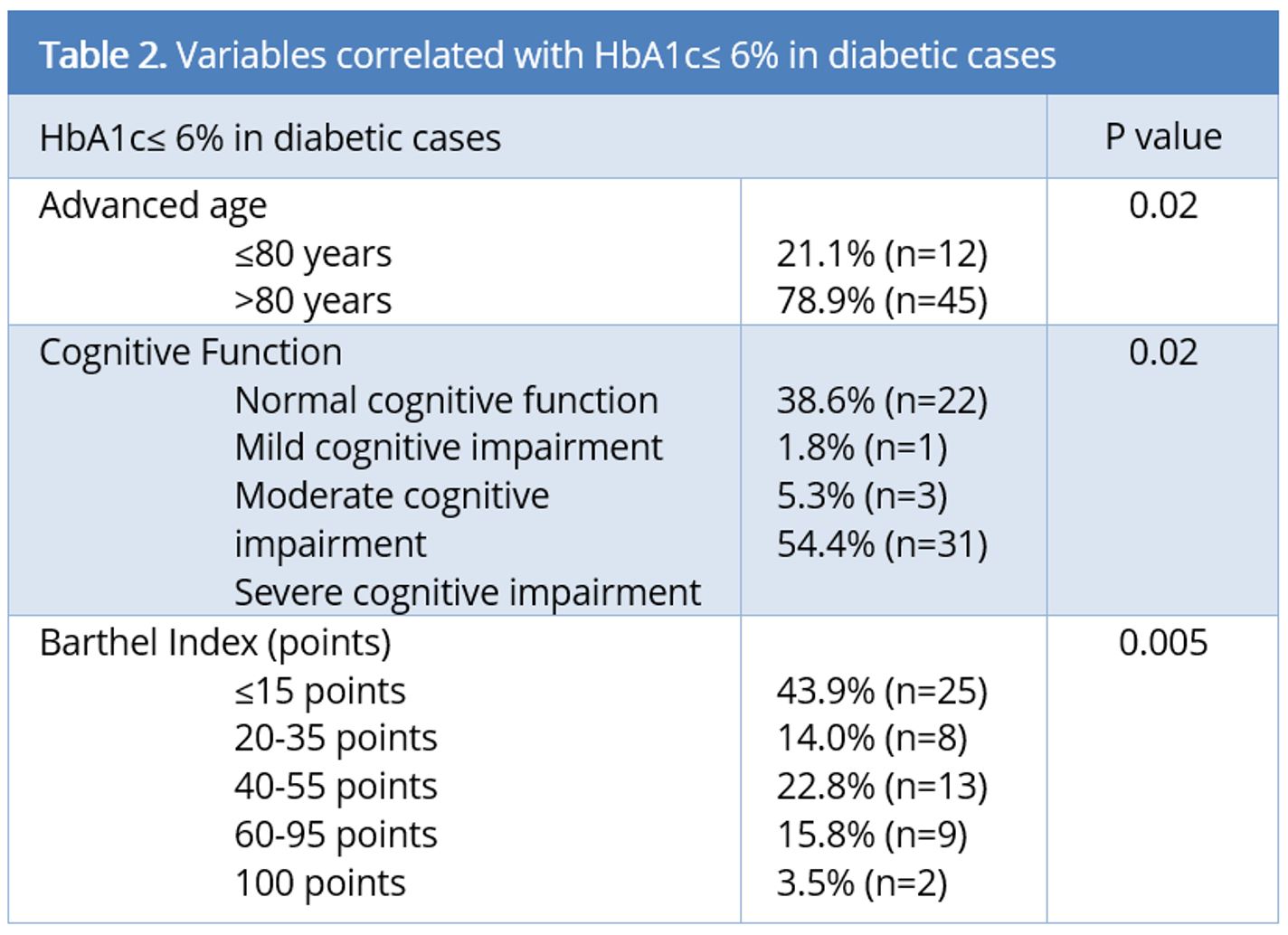
Advanced age (P = 0.02) and moderate-severe cognitive impairment (P = 0.02) were the variables associated with an intense glycemic control and a high risk of developing hypoglycemia. In contrast, the non-diabetic group was not significantly associated with these outcomes (Table 2).
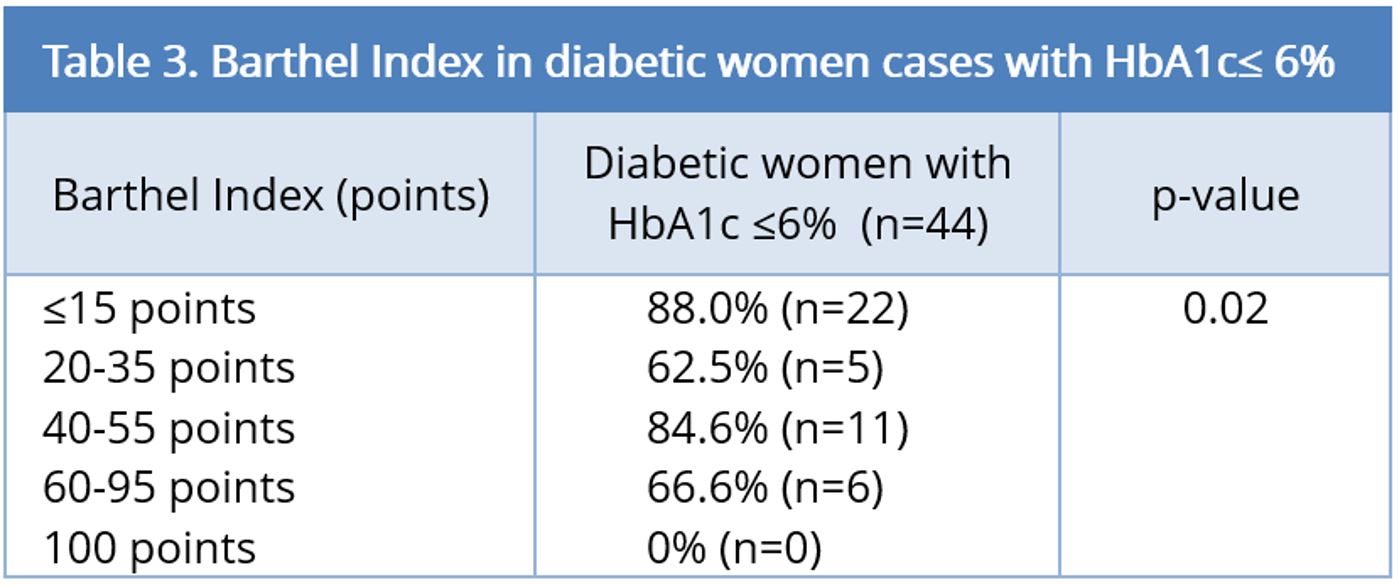
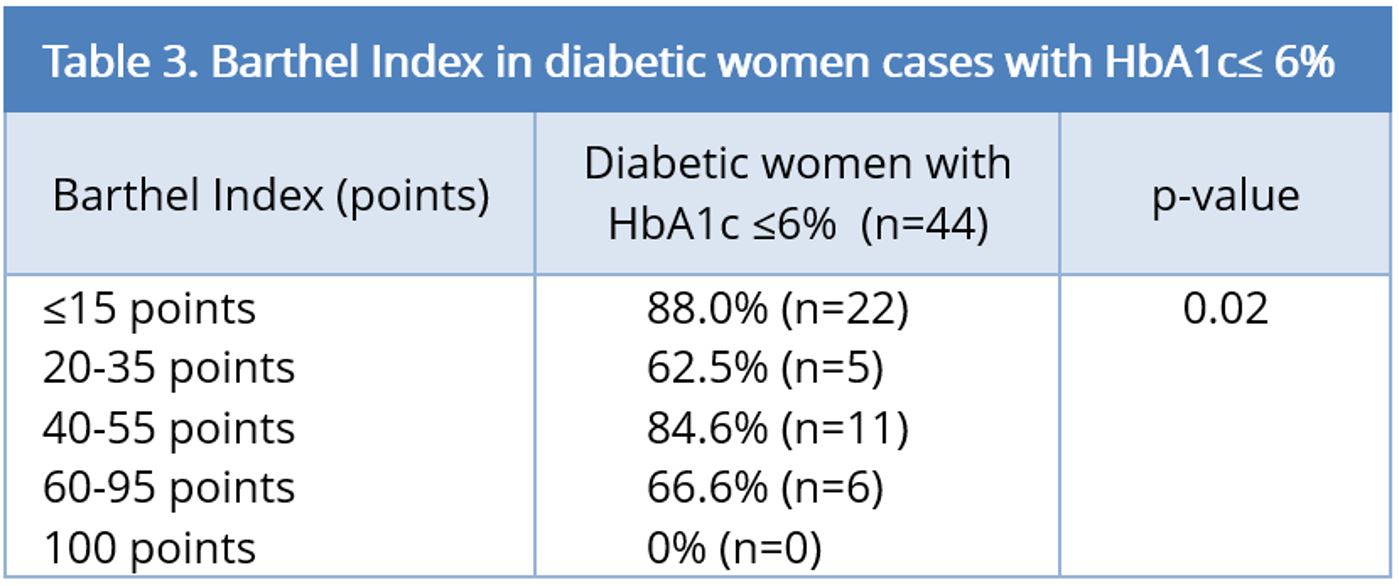
This study did not show an association between HbA1c low levels and general functional status (p.value > 0.05 in General Barthel Index), but it showed association between HbA1c low levels and functional dependence in female diabetic patients (P = 0.02) (Table 3). Low scores in the Barthel Index were also associated with a high risk of developing hypoglycemia (P = 0.005).
In this research, we studied the relationship of T2DM with cognitive impairment in the population living in nursing homes in Galicia (Spain). T2DM prevalence was 23.5%. These results show that T2DM prevalence is high compared with the community, according to a variety of studies that indicate a prevalence between 10-20% [17-19], but similar to that found in geriatric population studies.
Most cases were women, who presented with worse cognitive status and higher physical dependence than men. In this study, females with low HbA1c levels have functional dependence correlation, but not in males. This mechanism could be possible because females have a longer age than males, and advanced age is associated with a higher functional dependence and maintaining low blood glucose levels for a long time. The Pfeiffer test was selected as the scale to assess cognitive status. It has sensitivity close to 70% and a very high specificity close to 95%, being a fast screening tool to evaluate cognitive changes. Our study did not attempt to diagnose dementia, for which more tools were needed. We wanted to know the degree of cognitive deterioration. For this purpose, the Pfeiffer test was an adequate indicator, as it had been validated and clinically contrasted. Besides, different experts in the field of geriatrics have agreed on using simple tests that require little time for their realization, especially for screening; and the Pfeiffer test meets these requirements [20].
Elderly people with diabetes are vulnerable to hypoglycemia with the development neuroglycopenic symptoms like confusion and disorientation. Hospital admissions due to severe hypoglycemia are 40% higher than those for hyperglycemia in geriatric patients [21,22]. Patients with dementia or cognitive impairment were significantly more susceptible to hospitalization as a result of hypoglycemia than the patients with normal cognitive function [6,23]. Hypoglycemia associated with diabetes treatments with secretagogues or insulin is more frequent and more severe in the elderly and has potentially serious consequences, such as falls, cognitive impairment, arrhythmias or cardiovascular events [24]. The elderly treated with insulin have a higher risk of cognitive impairment and dementia because they have a long disease evolution and have a suboptimal control of glycemic targets [21]. The results of our study show a link between the treatment with insulin and a higher rate of severe cognitive impairment compared to the treatment with oral antidiabetics where no association was found.
Cognitive impairment and dementia constitute an important health problem in the geriatric population. In particular, the elderly diabetics presented with recurrent hypoglycemia have higher mortality rates and an increased risk of cognitive decline and dementia. Moreover, the brains of the elderly population are more vulnerable to the effects of these hypoglycemias.
We found that more than half of the diabetic patients had HbA1c values below 6.5%, and only 23.4% of them had levels between 7% and 8.5%, which was recommended by the different international associations as good control in this frail and complex population [9]. These findings demonstrate a potentially harmful aggressive hypoglycemic therapeutic approach in these patients. Therefore, specific treatment strategies should be proposed for glycemic control to limit metabolic decompensation and avoid the risk of hypoglycemia, and HbA1c targets under 8.5% are made acceptable for older adults with multiple comorbidities and limited life expectancy [25]. In our study, HbA1c levels were lower in demented patients, who were more prone to the consequences of hypoglycemia; there were signs of overtreatment in the population as a whole. Cognitively impaired and demented patients are more vulnerable to hypoglycemia, which itself represents a major risk factor for further cognitive decline [5,6,12,24]. Atypical clinical presentation of hypoglycemia makes an early diagnosis of hypoglycemia and their harmful consequences are extremely difficult in demented and frail patients.
Our results demonstrate that there could be an association between the levels of HbA1c < 6% in diabetics and severe cognitive impairment. The latest recommendations of the American Diabetes Association [10] establish that older adults have a high risk of hypoglycemia, citing high morbidity, insulin therapy or progressive renal failure among the causes of such increased risk. In addition, with aging, the cognitive deficit rates increase, leading to a deterioration of self-care, poor glucose controls or insulin dose adjustment.
These deficits have been associated with an increased risk of hypoglycemia; and severe hypoglycemia is associated with an increased cognitive impairment proportion. It is necessary that all healthcare teams identify any cognitive status modification in diabetic patients, emphasizing the importance of hypoglycemia prevention. Similarly, antidiabetic treatments need to be adapted to the needs and daily activities of this complex population [16,26]. The objectives of glycemic control should be patient-centered and individualized in each case, instead of trying to achieve strict control of HbA1c levels.
Furthermore, a meta-analysis published in 2016 shows the bi-directional relationship between cognitive impairment and hypoglycemia in older patients and concludes that glucose-lowering therapy should be carefully tailored and monitored in older patients who are susceptible to cognitive decline [27].
The objective treatment according to different guide experts should be directed to the symptoms relief, preventing long-term complications, and avoiding hypoglycemia. The functional status of each patient should be determined, with special emphasis on the presence of cognitive impairment or dementia, where HbA1c targets should be around 8.5% [21].
All health personnel working at nursing homes centers should pay attention on identifying both physical and cognitive modifications in diabetic patients, anticipating hypoglycemias or any other symptomatology related with T2DM, and suitable treatment to their daily activities and needs, rather than aiming at a specific HbA1c [26].
As study limitations, we found that age was a risk factor for cognitive decline in the HbA1c < 6.5% group. However, there was the possibility that these patients had HbA1c < 6.5% for longer time than their younger counterparts, indicating that the correlation with cognitive decline might be age or maintaining low blood glucose levels for a long time.
In this cross-sectional study, no previous information regarding glucose levels before the study was collected and no analysis was performed to determine which variables were associated with rigorous T2DM control and the risk of developing hypoglycemia. This was a limitation to our work, which would have provided important information about glycemic control and its complications.
The management and treatment of the studied institutionalized geriatric diabetic population in our region could be too strict. Consequently, hypoglycemia in these patients could play a role in the major decline of cognitive function. Diabetes control should be determined by the level of fragility, physical dependence and cognitive status, adjusting glycemic control objectives to this situation. In addition, the healthcare teams at home nursing centers should receive specific training to deal with diabetes and cognitive impairment that is adapted to this stage of the life cycle.
Received date: August 17, 2017
Accepted date: October 16, 2017
Published date: December 16, 2017
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
The authors declare no financial and personal relationships with other people or organizations with any interest finan-cial or otherwise in the subject matter discussed in this manuscript.
The authors wish to thank to the residents and professionals who have participated in this study, and managers of the centers for their collaboration.
© 2017 The Author (s). This is an open-access article distributed under the terms of the Creative Commons Attribution 4.0
Radiation forms a vital part of neoadjuvant treatment in locally advanced rectal cancer (LARC) and recurrent rectal cancers. The adverse effects of radiation are well recognized; however, radiation-induced perforation at the tumour site is very rare and is poorly understood. A symptomatic rectal perforation requires an emergency surgical intervention. However, it may present silently and can give rise to suspicion of disease progression and/or residual disease on imaging. Authors present two cases of silent perforations. Both gave rise to a considerable diagnostic dilemma, which was resolved by careful evaluation with MRI.
This pilot study compares the agreement in diagnosis between scanned slides and conventional microscopy in both low and high magnifications.
Smartphones and cellular technology have revolutionized flap monitoring. Smartphones provide low-cost thermal imaging alternatives to flap monitoring. It remains unclear, however, whether this method is accurate or reliable. It may be challenging to use smartphone thermal imaging when clinicians fail to communicate clinically relevant events. The authors demonstrate three instances in which the thermal imaging information on smartphones was misleading. Each case is analyzed to determine how clinical decisions should be made.
The article discusses a complex case of a 51-year-old Chinese woman diagnosed with a pituitary neuroendocrine tumor in the clivus, characterized by its invasive nature and atypical symptoms, leading to diagnostic challenges between chordoma and chondrosarcoma. Achieving a correct diagnosis through a transsphenoidal biopsy enabled effective surgical removal of the tumor without complications. Highlighting the critical role of biopsy for accurate diagnosis, especially with atypical imaging, the study showcases the efficacy of minimally invasive transnasal endoscopic biopsy techniques. It emphasizes the importance of a multidisciplinary approach for optimal patient outcomes in complex pituitary tumors, underlining the need for vigilance and adaptability in managing such rare conditions. This contributes valuable insights to the medical field, particularly for neurosurgery, otorhinolaryngology, and endocrinology practitioners.
The article stands out by providing a comprehensive analysis of a rare case of a midline branchial cleft cyst, a significant contribution given that only three other cases have been documented in medical literature. This scarcity underscores the article's value, making it a crucial read for medical professionals. It not only highlights the diagnostic challenges and treatment strategies for such atypical presentations but also enriches the understanding of branchial cleft cysts beyond the common lateral neck occurrences. By including a detailed review and comparative analysis of these few reported cases, the article offers unique insights into the demographic, symptomatic, and anatomical variations of branchial cleft cysts. This focused analysis makes the article an indispensable resource for clinicians, surgeons, and students in the medical field, aiming to enhance diagnostic accuracy, inform clinical practice, and ultimately improve patient outcomes in dealing with complex and rare presentations of congenital anomalies.
This narrative review advances the management of radiation-induced dysphagia in head and neck cancer treatment by integrating advanced imaging, precision dosimetry, and structured rehabilitation. Beyond focusing solely on dysphagia-optimized intensity-modulated radiotherapy, it explores a variety of approaches: MRI and CT provide detailed anatomical insights, while proton therapy offers a less toxic alternative, and early rehabilitation preserves swallowing function. This holistic model prioritizes patient quality of life, detailing how techniques like Do-IMRT reduce radiation to critical structures like the pharyngeal constrictors and larynx, maintaining effectiveness. The review advocates a multidisciplinary approach, encouraging collaboration among oncologists, radiologists, and therapists to enhance long-term patient well-being and promoting further research to elevate care standards.
Major Comments/Concerns
Minor Comments/Concerns
Major Comments/Concerns
Minor Comments/Concerns
Accept for publication.
The authors stated that they used multivariate regression analysis, but actually they only used "cross tabulation" or "Chi-Square analysis". If the authors failed to use the multivariate analysis, please delete the description of multivariate analysis and please mention this study limitation in the discussion section (study limitation section).
ResponseDescription of multivariate analysis was deleted. The next limitation was added: In this cross-sectional study, no previous information regarding glucose levels before the study was collected and no analysis was performed to determine which variables were associated with rigorous T2DM control and the risk of developing hypoglycemia. This was a limitation to our work, which would have provided important information about glycemic control and its complications.
Carreiro Alonso MA, Mayán Santos JM, Iglesias Vilanova M, Pose Reino AD. Over effective control of glycemic levels could cause cognitive decline in diabetic geriatric population. Neurol Neurosci Res 2017;1(1):3. https://doi.org/10.24983/scitemed.nnr.2017.00047
 PDF
PDF