Bone, cartilage, muscles, subcutaneous layer, and skin form nasal tissues. Anatomy and physiology in young and normal individuals have been extensively studied and published; nevertheless, little importance has been focused on the concept of nasal aging and its related rejuvenation procedures. The former is a continuous process that may alter patient aesthetics, functionality, and self-esteem. Although corrections of this condition were not available in the past, modern science has developed minimally invasive alternatives that have attracted the interests of patients and medical community. The author presents a review of the principal aspects of nasal aging and an algorithm to approach nasal rejuvenation.
Anatomical nasal tissues include bone, cartilage, muscles, subcutaneous layer, and skin. All these elements are carefully organized to allow proper physiology and adequate aesthetics. These variables have been extensively studied and published, principally related to the corrections of development or post-traumatic abnormalities. Nasal surgical corrections have focused on re-establishment of normal function and anatomy. Patients seeking nasal surgical corrections are generally young individuals [1]. The former has influenced little interest and development of the concept of nasal aging and its related rejuvenation procedures.
Nevertheless, since 2008, Braccini’s concept of medical rhinoplasty has expanded the armamentarium available for the treatment of nasal conditions and the universe of the patients seeking corrections [2]. Although the majority of patients seeking medical rhinoplasty are young individuals, there is a new trend in a number of adults and older patients requiring minimally invasive nasal corrections. The study of nasal aging becomes vital prior to nasal rejuvenation procedures.
Nasal aging includes skin aging and related tissues aging. Skin aging comprises of chrono aging and photo aging. Photo aging is related to the sun UV-exposure and is highly preventable. Changes in the skin due to sun damage include elastosis, melanin disorders (hypo/hyper pigmentation), and premalignant and malignant conditions.
Chrono aging happens due to the passage of time and generally includes skin thinning or thickening, depending on the case, and sebum and hydration variations. The rosacea related disorder manifests in the nose as telangiectasia and vascular development, ostium follicularis, and skin enlargement that may determine the apparition of rhinophyma [3].
This genetically determined condition can worsen by external factors such as heat or alcohol, being the natural progression, the enlargement of vessels and dermic components, which become the real stigma of the disease, and at advanced stages, become independent of external stimuli.
Related tissues of the nose are also prone to aging. Generally, with the passage of time, the adipose tissue tends to atrophy, especially in the region of the glabella and root, and also in the dorsum and tip. The former affects directly the exposure of deeper tissues, such as cartilage and bone, which get superficial, giving the nose a skeletonized aspect. This phenomenon is particularly important in pre-existent thin soft tissue patients, especially females. Nasal muscular components are also prone to aging and may extent in time [4].
The cartilage component experiments a continuous growth of medial and lateral crura, affecting dome projection and rotation. On the contrary, caudal septum tends to reabsorb in time. These events, although non-exclusive, are more prominent in males, which manifest thicker and heavier tissues [5-6]. The bony aspect of the nose experiments enlargement of the piriform aperture and reabsorption of the anterior nasal spine points, where the whole structure of the nose is anchored [7-10].
All of the above aspects determine the visual detachment of the nose from the face, as the superior and inferior thirds of the nose are under-projected. The nose tip typically becomes larger with a loss of tip defining points, support, projection, and rotation. Furthermore, there is a flattening of the supratip break.
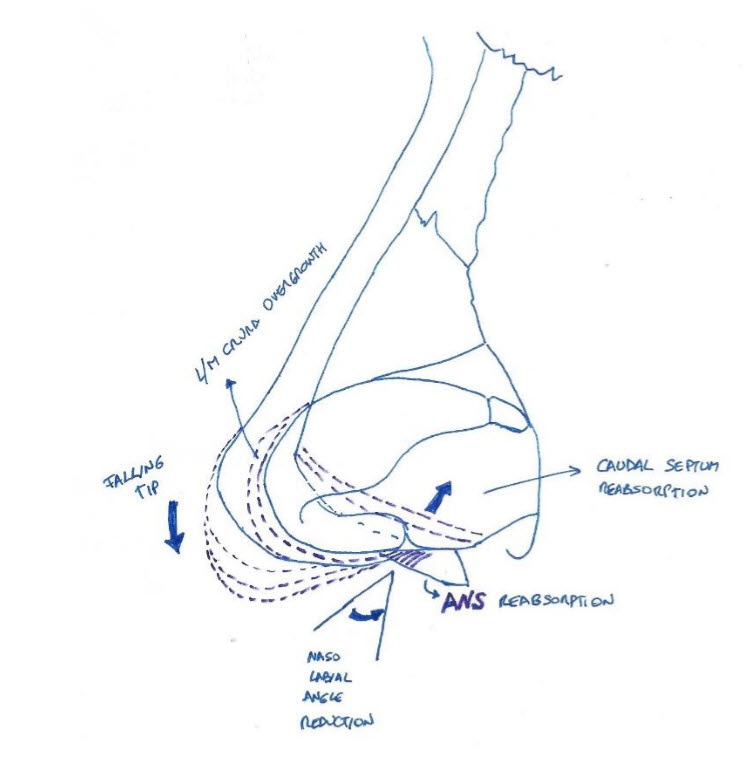
Clinically, the frontal view of the aging nose has a reduced vision of the nostrils and retracted or hidden columella. Lateral views show a reduction in the nasolabial angle that is typically below 85 degrees in males and 90 in females. All the former changes are shown in Figure 1.
As nasal structures, age physiology [11] and sensitivity [12] may alter, indicating that this process is not just an aesthetic problem.
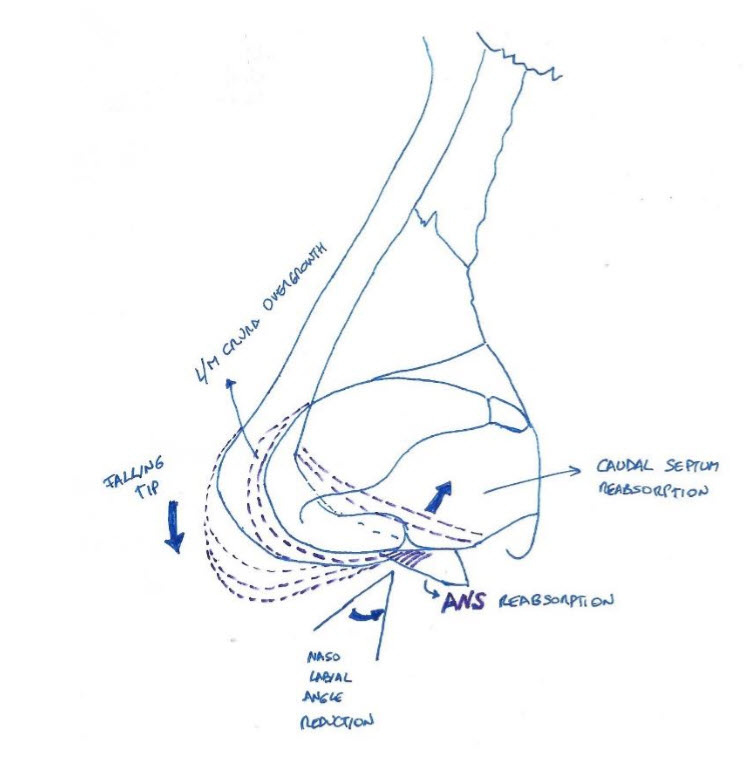
Figure 1. Physiopathology of nasal aging.
Facial & Nasal Rejuvenation
Classical facial rejuvenation procedures are focused more on improving the external part of the facial oval, being more concerned about the surgeon’s skills than on patient’s needs. The principal facial traits are located in the center of the face and so is the related importance for patients looking for corrections [13]. The former has shifted the aesthetic procedures to a centripetal approach, giving more importance to the eye frame area and nasal procedures. Although surgical rhinoplasty alone can induce dramatic rejuvenating changes in the face [14], combination techniques grant a more natural and global correction [15]. Nevertheless, the dramatic changes and downtime of a surgical procedure are not always what an elder patient seeks [1].
The contemporary concept of minimally invasive nasal rejuvenation has become lately a matter of interest for patients and physicians due to a concrete aesthetic and functional improvement with no downtime. Moreover, it has become a frequent topic in recent international aesthetic meetings, being considered as one of the last frontiers in facial rejuvenation.
Nasal Rejuvenation Procedures
Prior to 2008, the only available treatments in the nose were surgical. In that situation, mostly young individuals were seeking for nasal corrections. Older patients were not prone to big surgical approaches that would give them a very different appearance. Moreover, their tolerance to swelling, inflammation and downtime decreases as they get into the productive phase. After Braccini’s publication, with the introduction of nasal fillers and botulinum toxin, a completely new era of soft nasal beautification techniques became available [2].
Very controversial on their introduction, they induced more and more interest among the patients seeking for nasal improvements due to lesser invasiveness and downtime.
These treatments were mainly performed over young or middle-aged individuals, and the techniques available were rudimentary and with a high risk of potentially devastating complications [16-20].
With the apparition of Nasal Torres No-Touch technique in 2015, and the introduction of curved cannulas, the repertoire available for nasal corrections widened and the incidence of adverse events dropped dramatically [21]. The former allowed the extension of these corrections to older patients who were not just looking for beautification, but to expand their use into nasal aging. The former enlarged the universe of the patients seeking nasal corrections and allowed to propose nasal corrections to patients who otherwise would not have gotten one.
The author has a series of 150 patients above 45 years, where all these concepts are applied. The principal techniques used in nasal anti-aging include cosmetics, rhinofillers, botulinum toxin, fat grafting, lasers, threads, and sutures [22].
Topical preparations applied over the nose can improve hydration and sebometry, reduce fine wrinkles and lines, even the pigmentation, and also reduce dilated ostium follicularis. The principal active ingredients used include retinoids and chemical peels agents. Their usage requires constant exposure and time, as the results are seen only after 3 months [23].
Rhinofillers
The term ‘medical rhinoplasty’ or ‘rhinofiller’ defines the application of dermal fillers in the external or internal nasal area to modify or improve aesthetics or functionality [24].
It is especially suitable for patients with minor aesthetic or functional concerns that are refractory to surgery [25]. It may be combined with the use of botulinum toxin injections around the nose to enhance the results. The procedure is currently a frequent request in aesthetic practice, and many physicians perform it systematically. Nevertheless, it is an advanced technique and should be attempted only by expert practitioners due to the possibility for devastating vascular complications and the potential need for complex reconstruction procedures [26]. Local anatomical knowledge and advanced technical skills are required to achieve successful and safe corrections.
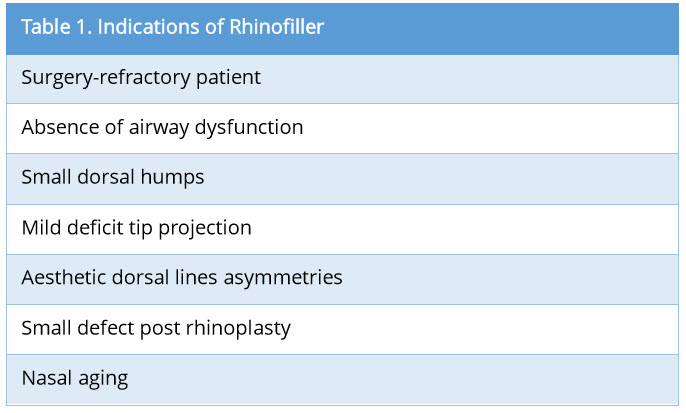
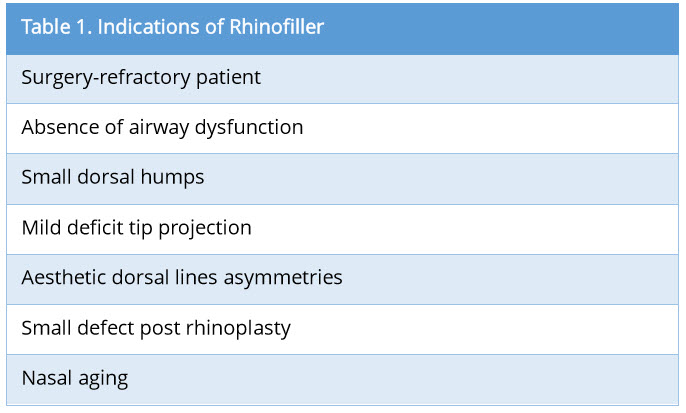
Rhinofiller is the infiltration of a dermal filler to modify external or internal nasal structures for aesthetic or functional purposes. Since its introduction in 2008, many different temporary or permanent substances have been used to achieve the desired corrections. Successful application mandates an adequate anatomical knowledge of the related structures. Proper patient selection is important to achieve good results. Exclusion criteria include severe nasal airway impairment, permanent filler in the area, history of ischemic/thrombotic events or known hypercoagulability, local infection, or recent trauma. The indications of rhinofiller are many, including the treatment of nasal aging (Table 1).
The fillers around the nose can be a powerful weapon to re-establish volume loss, especially in the radix or base. Moreover, they can favor an increase in the nasolabial angle lifting the nose tip and reversing the tip ptosis. The former is achieved with the tripod volumetric graft (previously published by the author), with the aid of curved cannulas.
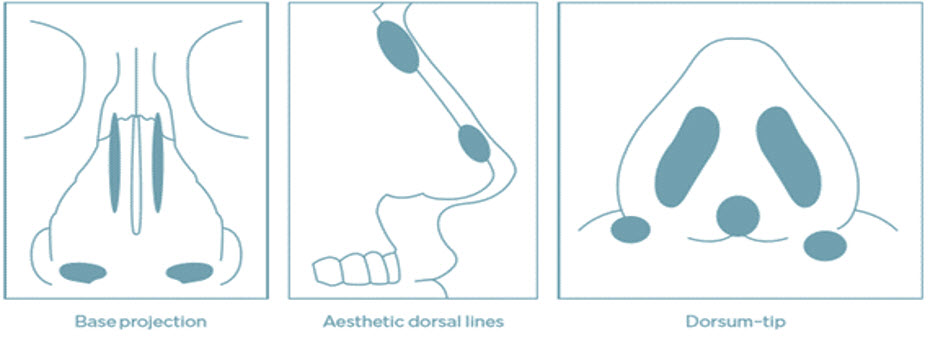
Before the procedure, the nasal analysis should be performed clinically and photographically to define necessary corrections. Areas of potential corrections include aesthetic dorsal lines, dorsum, minor hump camouflage, radix enhancement, tip rotation and projection, and base augmentation. The detail is shown in Figure 2.
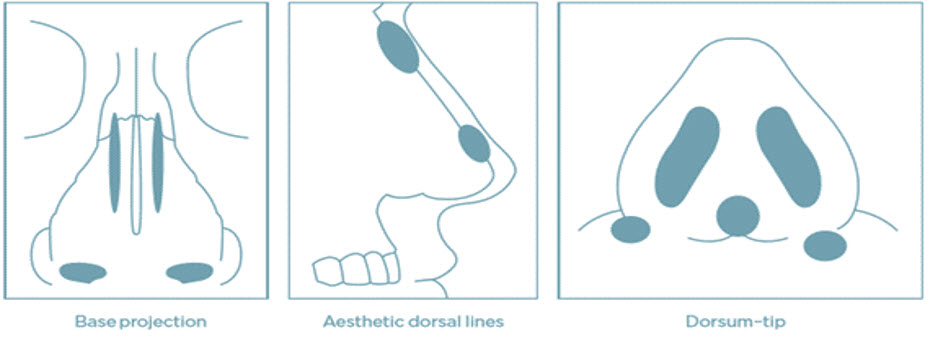
Figure 2. Areas of potential fillers corrections.
Functionally, in selected cases, the use of fillers can be beneficial to augment the aperture of the internal nasal valve as a volumetric spreader graft.
Morphing simulations are advisable before the treatment in order to give the patients an indication of the post-treatment outcomes, explain the procedure, and establish common goals. In addition, specific informed consent should be properly discussed and obtained.
Technique
Treatments are typically performed with medium viscosity hyaluronic acid fillers, under local anesthetic (lidocaine intradermal vesicles applied using a 0.3 ml syringe with a 32 G needle) with the aid of a 25 G (0.5 mm) × 4 cm blunt-tip, disposable cannula, manually bent, maintaining sterility at all times, in order to obtain a better compliance of shapes and silhouette within the nasal area. The distribution of material should be performed as required to follow the treatment plan. Tip refinements can be sporadically carried out through needle infiltration with extreme care.
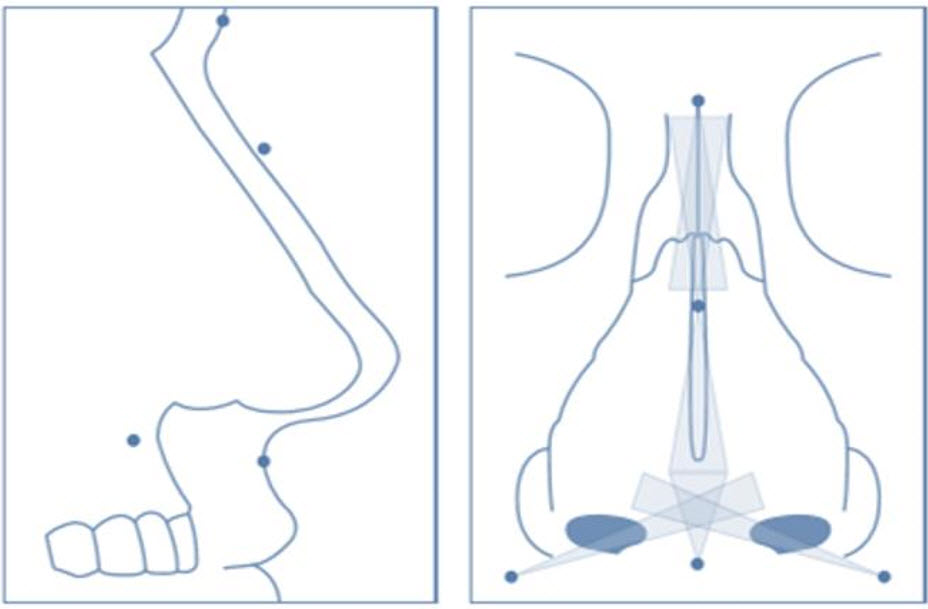
The specific pattern of anesthetic peripheral blocks and filler infiltration is shown in Figure 3.
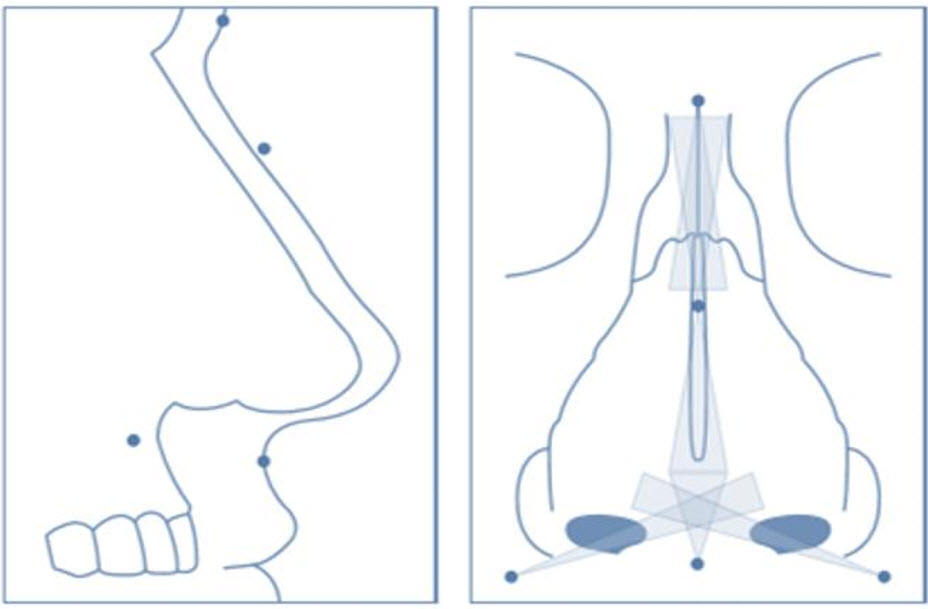
Figure 3. Perispheral anesthetic blocks and filler distribution.
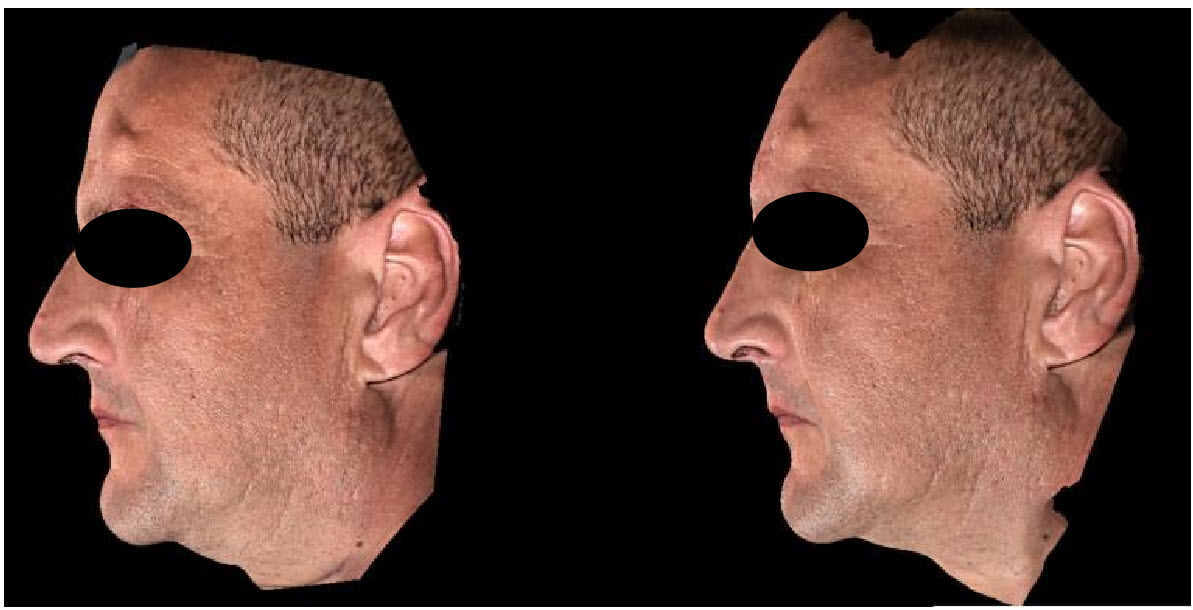
Generally, patient satisfaction rate with this correction is very high. Due to the scarce muscular activity in the nose, corrections with Hyaluronic acid dermal fillers last above 1 year, and in many cases even two. Rhinofiller clinical cases are shown in Figures 4-6.

Figure 4. Lateral view of nasal rejuvenation with fillers, Hyabell® Basic 16mg/ml produced by Adoderm, Germany. Notice straight dorsum, and change in nasolabial angle.

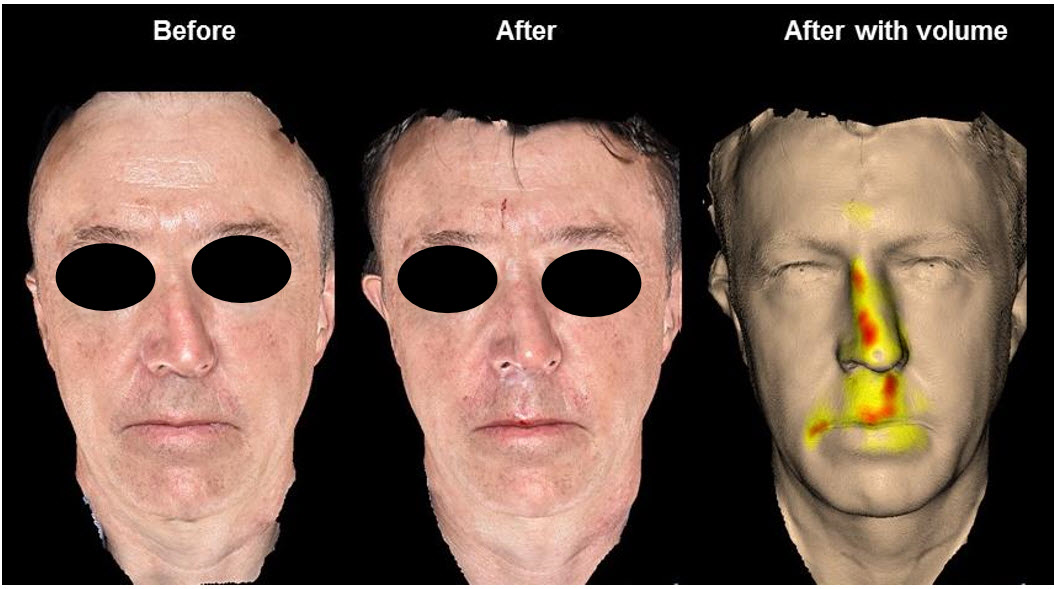
Figure 5. Frontal view of nasal rejuvenation with fillers, Hyabell® Basic 16mg/ml produced by Adoderm, Germany. Notice the changes in nostrils area exposure.
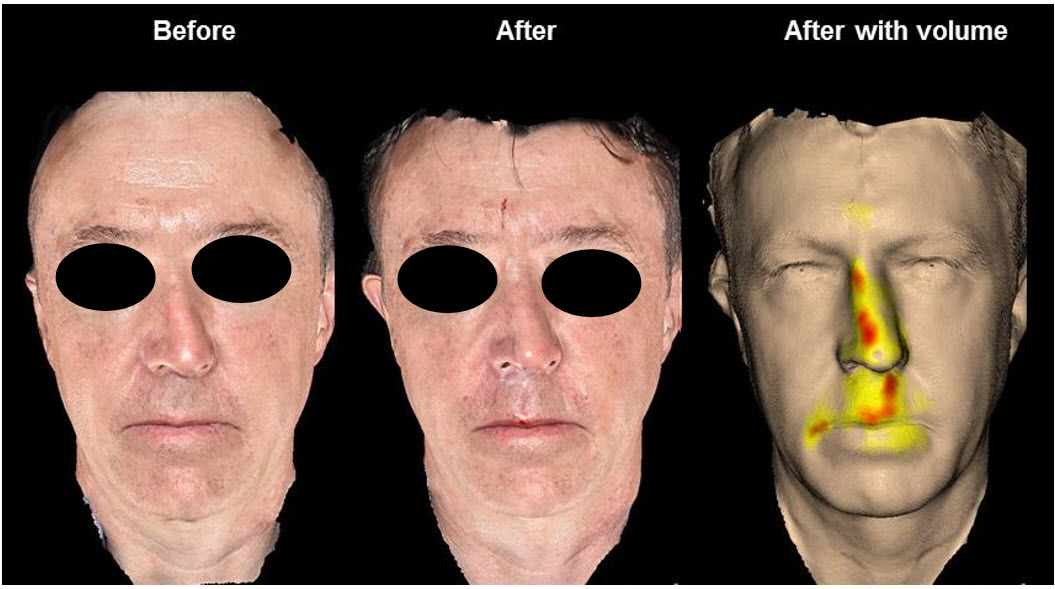
Figure 6. Frontal view of nasal rejuvenation with fillers, Hyabell® Ultra 24mg/ml produced by Adoderm, Germany. Notice the important nasal deviation corrected after the volumization and the colorimetry design that shows the areas of filler placement.
All of the above have determined nasal augmentation with dermal fillers to be particularly challenging. Mastery of the correct technique is of utmost importance in order to achieve good results and reduce the incidence of adverse reactions.
Nasal Botulinum Toxin
The onset of the neurotoxin in aesthetics revolutionized the treatment of dynamic facial wrinkles, producing a reversible paralysis that allows overlying tissues to relax and to be aesthetically flattened and raised. The use of botulinum toxin around the nose differs from the typically recommended indications of the superior facial third, being considered an advanced and off-label technique. The use of botulinum toxin in the nose is useful in hyper-motile noses that typically move with mimic expression. The complications related to this technique are not as severe as the use of rhinofiller, because they are reversible and do not affect nose vascularity. Complications include pain, bruising, swelling, asymmetries, short lasting effect, and resistance. Lasting of the corrections is limited (3-4 months) and the action takes 2-10 days to establish; but, it may enhance the results obtained with a rhinofiller, as it removes muscular action and tension over the nasal region. Deep punctures at a muscular level are necessary. The muscles suitable for being treated around the nose are as follows:
Nasal Lasers
CO2 Lasers can be extremely useful for the treatment of severe skin hypertrophy such as in rhinophyma. Local anesthetics and sedation are necessary, and adequate postop skin care, as well as herpes prophylaxis, must be given as healing time can be prolonged.
Vascular lasers, such as Ndyag, Dye, KTP or Copper, can be used to treat vascular overgrowth. Tolerance to the procedure is generally good and topical anesthetics are sufficient in most cases. More than one session may be required.
Nasal Fat Grafting
Nose lipofilling can be a valid alternative for nasal reconstruction as they can expand the tissues volumetrically with a permanent effect and bene fit the tissues due to the regenerative actions of the stem cells within the fat. This can allow further more invasive reconstruction techniques, as the tissues recover from previous damages.
Micro or Nano grafts can be delivered with a technique similar to rhino fillers.
Threads & Sutures
Threads are surgical filaments of generally reabsorbable (PDO, poly lactic acid) materials with self-anchoring characteristics that may lift the tissues and stimulate collagen overgrowth. As the threads are free, their traction action relies mainly on the tines they have along. They have been used to stimulate volumization through collagen overgrowth, straighten the dorsum and to promote lifting of the tip. Unfortunately, the results are usually short-lasting (3-5 months) as the most ptotic noses are generally bigger with thicker skin, and heavier.
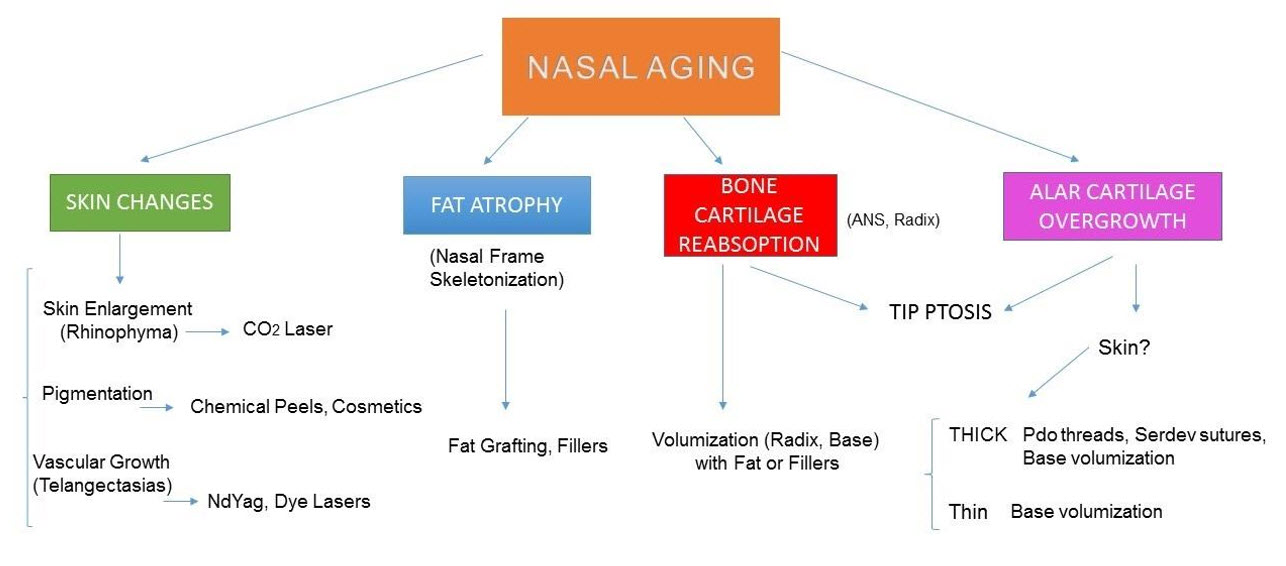
On the other hand, nasal sutures are made out of reabsorbable semi-elastic, braided material (polycaproamide) with deep periosteal anchoring point, the presence of a tie and a knot, that grant greater duration and effect than the threads. The treatments require local anesthetics, sedation, and the knots should be performed under medium tension to prevent exaggerated and unnatural effects. An algorithm to nasal aging and rejuvenation is presented in Figure 7.
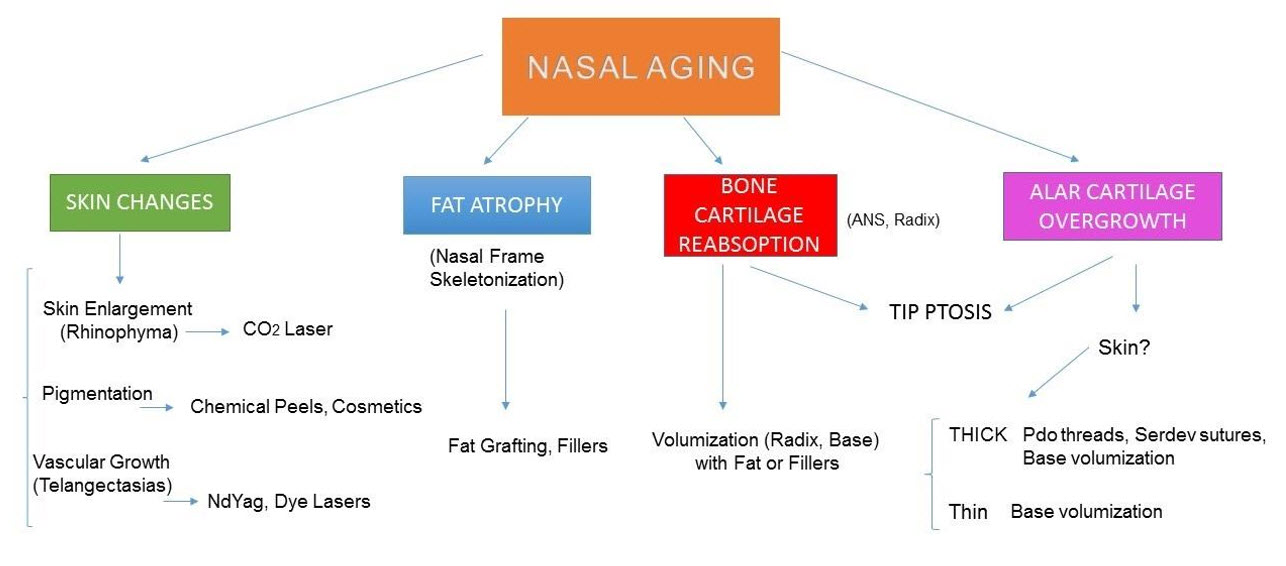
Figure 7. Algorithm of Nasal Aging and Rejuvenation.
Nasal aging is a continuous process that may alter the organ aesthetics and physiology, causing great distress to patients. Current nasal rejuvenation techniques allow minimally invasive corrections with minimum downtime, consistent and natural results, and should be in the armamentarium of trained specialists.
Received date: July 05, 2017
Accepted date: August 03, 2017
Published date: August 23, 2017
© 2017 The Author. This is an open-access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC-BY).

Figures section: While preparing the manuscript, please make sure that you are citing the figures at the relevant places in the text. If images of patients are used, either the subjects should not be identifiable or their pictures must be accompanied by written permission to use the figure.
Tables section: Begin each table on a separate page. Tables must be submitted in Word table format. Tables should be placed on separate pages and be numbered in the proper order of their mention in the text. Provide a brief title for each table, and define any abbreviations in table footnotes.
References section: The authors are responsible for the accuracy and completeness of their references. Each reference should be identified in the text in numerical order and should be identified by superscript Arabic numerals.
Response Thank you for your comment. We have added references to the paper.The revisions made by the author have improved this paper considerably. It can be accepted for publication.
The author has made the correction as suggested particularly citing the references within the text. This article can be accepted for publication.
Torres S. Nasal aging and rejuvenation. Arch Otorhinolaryngol Head Neck Surg 2017;1(2):3. doi:10.24983/scitemed.aohns.2017.00026
 PDF
PDF