A 33-year-old female with an unremarkable medical history presented to the clinic with concerns about the acute onset of right-sided facial swelling accompanied by severe pain, dysphonia, and dysphagia. The patient reported a history of chronic pain associated with the lower right first molar. She had received a root canal treatment on the same tooth one month prior to presentation. On the night before her visit, she noticed facial swelling that rapidly progressed overnight and was accompanied by severe pain radiating to her right ear, which prompted her to seek medical evaluation. Furthermore, the patient noted new-onset difficulties swallowing solids and liquids, as well as speaking full sentences. Further evaluation and diagnostic imaging were ordered to investigate the cause of these symptoms.
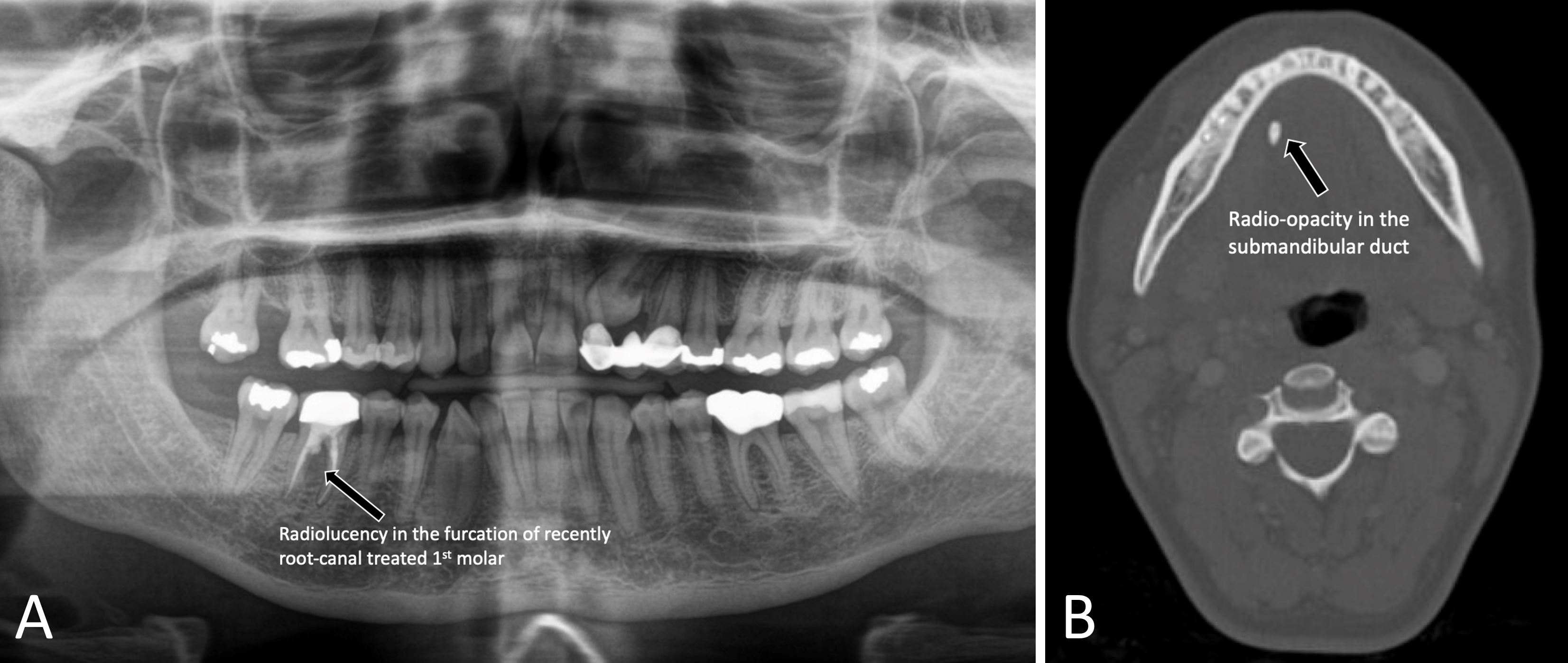
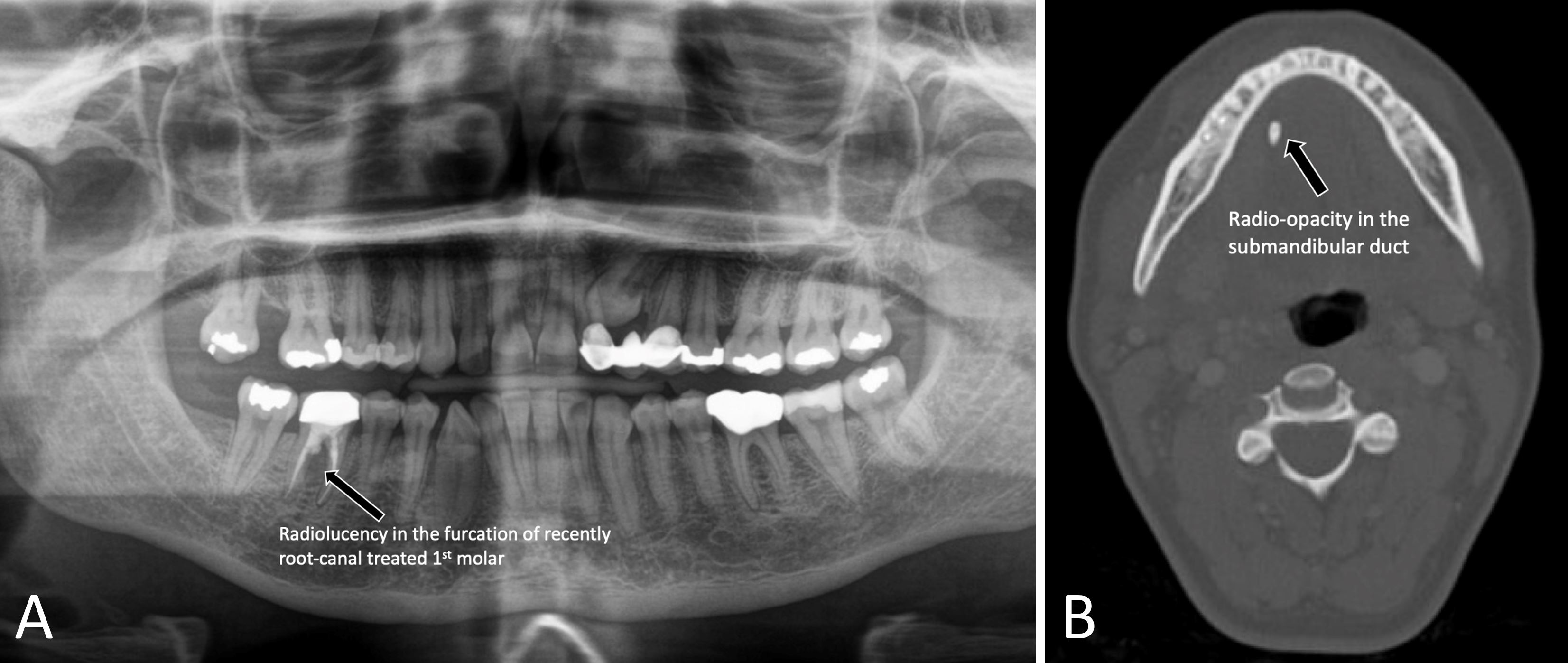
The patient exhibited stable vital signs during examination. The presentation included facial swelling overlying the inferior border of the mandible, extending from the ramus anteriorly to the body of the mandible. On examination, the patient displayed a satisfactory level of mouth opening. Intra-oral examination revealed a raised floor of the mouth, which was tender upon palpation, along with fluctuation and induration. The patient's voice was strained and soft. Panoramic imaging showed a radiolucency associated with the previously treated tooth (Panel A), indicating an odontogenic abscess in the setting of failed root canal treatment. These clinical and radiographic findings prompted further evaluation and treatment, and the patient was referred to the emergency department for additional work-up and intravenous antibiotics.
At the emergency department, a flexible fiberoptic nasopharyngolaryngoscopy was performed at the bedside by an otolaryngologist. The examination revealed a patent airway without any notable findings. Subsequently, neck computed tomography imaging with contrast was carried out, which demonstrated radio-opacities along the right submandibular duct's course. Accompanying fat stranding was observed overlying the right mandible, without any indication of fluid collections (Panel B). Based on these results, sialolithiasis was deduced to be the most plausible diagnosis. Upon discharge, the patient was prescribed a course of antibiotics containing Amoxicillin-potassium clavulanate (Augmentin), sialagogues, and warm compresses. Following a two-week follow-up, the patient claimed near-total recovery after the passage of a salivary stone.
Upon initial evaluation, concerns were raised about a rapidly advancing odontogenic abscess that had the potential to invade the submandibular and neck spaces, posing a risk to the airway. Consequently, immediate or emergent care was deemed necessary, including incision and drainage, as well as odontectomy for source control. However, this case demonstrated that sialolithiasis may present in a similar fashion due to its proximity to adjacent structures. Therefore, the clinical presentation may resemble that of an odontogenic abscess. This case underscores the importance of keeping anatomic structures in mind when establishing a differential diagnosis. It also emphasizes the significance of avoiding tunnel vision when looking for the likely cause of clinical presentation.
Received date: February 26, 2023
Accepted date: March 02, 2023
Published date: March 08, 2023
The manuscript has not been presented or discussed at any scientific meetings, conferences, or seminars related to the topic of the research.
The study adheres to the ethical principles outlined in the 1964 Helsinki Declaration and its subsequent revisions, or other equivalent ethical standards that may be applicable. These ethical standards govern the use of human subjects in research and ensure that the study is conducted in an ethical and responsible manner. The researchers have taken extensive care to ensure that the study complies with all ethical standards and guidelines to protect the well-being and privacy of the participants.
The author(s) of this research wish to declare that the study was conducted without the support of any specific grant from any funding agency in the public, commercial, or not-for-profit sectors. The author(s) conducted the study solely with their own resources, without any external financial assistance. The lack of financial support from external sources does not in any way impact the integrity or quality of the research presented in this article. The author(s) have ensured that the study was conducted according to the highest ethical and scientific standards.
In accordance with the ethical standards set forth by the SciTeMed publishing group for the publication of high-quality scientific research, the author(s) of this article declare that there are no financial or other conflicts of interest that could potentially impact the integrity of the research presented. Additionally, the author(s) affirm that this work is solely the intellectual property of the author(s), and no other individuals or entities have substantially contributed to its content or findings.
It is imperative to acknowledge that the opinions and statements articulated in this article are the exclusive responsibility of the author(s), and do not necessarily reflect the views or opinions of their affiliated institutions, the publishing house, editors, or other reviewers. Furthermore, the publisher does not endorse or guarantee the accuracy of any statements made by the manufacturer(s) or author(s). These disclaimers emphasize the importance of respecting the author(s)' autonomy and the ability to express their own opinions regarding the subject matter, as well as those readers should exercise their own discretion in understanding the information provided. The position of the author(s) as well as their level of expertise in the subject area must be discerned, while also exercising critical thinking skills in order to arrive at an independent conclusion. As such, it is essential to approach the information in this article with an open mind and a discerning outlook.
© 2023 The Author(s). The article presented here is openly accessible under the terms of the Creative Commons Attribution 4.0 International License (CC-BY). This license grants the right for the material to be used, distributed, and reproduced in any way by anyone, provided that the original author(s), copyright holder(s), and the journal of publication are properly credited and cited as the source of the material. We follow accepted academic practices to ensure that proper credit is given to the original authors and the copyright holder(s), and that the original publication in this journal is cited accurately. Any use, distribution, or reproduction of the material must be consistent with the terms and conditions of the CC-BY license, and must not be compiled, distributed, or reproduced in a manner that is inconsistent with these terms and conditions. We encourage the use and dissemination of this material in a manner that respects and acknowledges the intellectual property rights of the original author(s) and copyright holder(s), and the importance of proper citation and attribution in academic publishing.
Authors report a young girl with an HNF1β mutation, who had a history of neonatal cholestasis, persistent liver dysfunction, and developed insulin-dependent diabetes without renal involvement. Further, authors review the literature related to the hepatic involvement associated with HNF1β mutations.
The clinical significance of otitis media with effusion (OME), a complication associated with cleft lip/palate (CLP), is often overlooked in children. The author reviews the pathogenesis, clinical manifestations, and diagnoses of OME in children with CLP as well as the controversies surrounding treatment. He also provides a flowchart to guide the management of OME in children with CLP.
The authors describe a 41-year-old man who suffered retraction-related complications that may have been missed or delayed. The present case illustrates the potential dangers associated with tympanic retraction pockets, despite the fact that their bottoms are clear and clean. The article discusses the reasons for the lack of consensus among otologists regarding the appropriate way to treat tympanic membrane retractions. There is further discussion regarding the challenges associated with early surgical intervention.
The patient was a 33-year-old female who presented with sudden onset facial swelling, pain, dysphonia, and dysphagia. Upon physical examination, swelling over the inferior mandibular border was observed, and panoramic imaging revealed radiolucency associated with a recently treated tooth, indicating an odontogenic abscess. A CT scan showed radio-opacities along the right submandibular duct, fat stranding over the right mandible, and an absence of fluid collections, consistent with sialolithiasis. The patient was treated with antibiotics, sialagogues, and warm compresses, and subsequently recovered after the discharge of a salivary stone. This case highlights the rare incident of sialolithiasis masquerading as an odontogenic abscess. It underlines the need for an exhaustive history, physical assessment, and radiographic examination to ensure a precise diagnosis and treatment. The manuscript has been exhaustively revised and complies with academic publication standards.
Kiang K, Sethi A. Looking beyond the obvious! A case of sialolithiasis masquerading as an odontogenic abscess. Arch Otorhinolaryngol Head Neck Surg 2023;7(1):2. https://doi.org/10.24983/scitemed.aohns.2023.00170
 PDF
PDF