Delirium is an acute disorder of arousal and attention that is commonly encountered, incompletely understood, and associated with adverse outcomes including increased morbidity and mortality, reduced health-related quality of life, and increased healthcare costs. In this narrative review, we examine the epidemiology, potential pathophysiological mechanisms, assessment, prevention, and treatment of this cognitive disorder. Delirium impacts up to 30% of hospitalized adults and most commonly affects patients with advanced age, cognitive decline, and medical or surgical comorbidity. While not fully understood, delirium is characterized by widespread dysfunction in inflammation, neurotransmitter and neurohormonal signaling, and structural abnormalities within the blood-brain barrier and brain parenchyma. Numerous screening assessments exist for delirium, but a clinical interview with cognitive examination is the gold standard for diagnosis. Prevention and early identification of delirium has the potential to be more effective than treatment of delirium, which requires the reversal of the underlying medical cause. Antipsychotic medications are used frequently for the management of acute agitation related to delirium, though there is little evidence for the efficacy of pharmacologic interventions. Further research into the pathophysiology, diagnosis, prevention, and treatment of delirium is greatly needed to reduce the incidence and sequelae of this common illness.
Delirium is defined as an acute disturbance of arousal, attention, and orientation, accompanied by disturbances in perception, emotion, memory, and psychomotor activity that is caused by an underlying medical illness or substance [1,2]. Although common, it is under-recognized, its pathophysiology is poorly understood, and treatment options are limited; moreover, it is associated with increased morbidity, mortality, and healthcare costs [3]. Despite increasing clinical interest in delirium, recent reviews have been limited in scope, focusing on either subtopic within delirium (i.e., diagnosis, prevention, treatment, etc.) or specific patient populations. Accordingly, we performed a narrative review of the literature focusing on the epidemiology, pathophysiology, diagnosis, prevention, and management of delirium across patient populations. This review summarizes the current understanding of delirium, highlighting recent advances in clinical approach, areas of uncertainty, and recommendations for management.
Incidence and Prevalence of Delirium
Delirium is a common syndrome that affects up to 30% of hospitalized adults [4]. The prevalence varies significantly depending on the patient population, as patients with advanced age, cognitive decline, and more severe medical illness are at higher risk. Most studies have explored delirium in the hospital setting and almost always in older individuals (e.g., > 65 years), rather than in the general population [5]. While relatively uncommon in the outpatient setting [6], delirium affects nearly 20% of patients over age 75 on medical inpatient units when formally assessed by experienced clinicians [7]. In intensive care unit (ICU) settings the prevalence is significantly higher, where rates of over 80% have been reported in mechanically ventilated patients [8]. Finally, among patients who have undergone surgery, the incidence of post-operative delirium ranges from 13% to over 50% [9,10]; a recent meta-analysis of 37 studies in patients over age 60 undergoing elective surgery found the pooled incidence of post-operative delirium to be nearly 19% [9].
It is notable that even within specific treatment settings, reported rates of delirium prevalence vary widely. For example, in the ICU setting, the prevalence of delirium has ranged from 20% to over 80% [8,11]. Some variability is likely attributable to study design (e.g., frequency of assessment), the method used to diagnose delirium (e.g., clinical evaluation vs. screening instrument), patient characteristics, and site-specific factors, such as practice patterns related to the use of sedative and analgesic medications [12].
Links Between Delirium and Health Outcomes
Delirium is associated with a multitude of adverse clinical outcomes, including longer time to extubation and increases in length of stay in both ICU [13] and general medical settings [14], thus putting patients at risk for additional medical complications associated with prolonged hospitalization [3]. Patients also face an increased risk of nursing facility placement or hospital readmission [3], and, following surgery, are also at increased risk of post-operative complications [9].
In the longer term, patients with delirium demonstrate accelerated cognitive and functional decline and an increased incidence of dementia [15]. Of greatest concern, elderly patients with delirium face increased mortality, with a meta-analysis finding a 95% increased hazard for mortality for delirious patients compared to non-delirious controls, even after adjusting for confounding variables [16]. Delirium is also associated with increased healthcare utilization, with estimated costs of between $16,303 to $64,421 per patient and an annual national burden of $143-152 billion per year in the United States [17]. These costs appear to primarily be related to prolonged hospitalization, higher costs per hospital day (e.g., longer ICU stay), and higher rates of nursing home placement and home health needs [17,18].
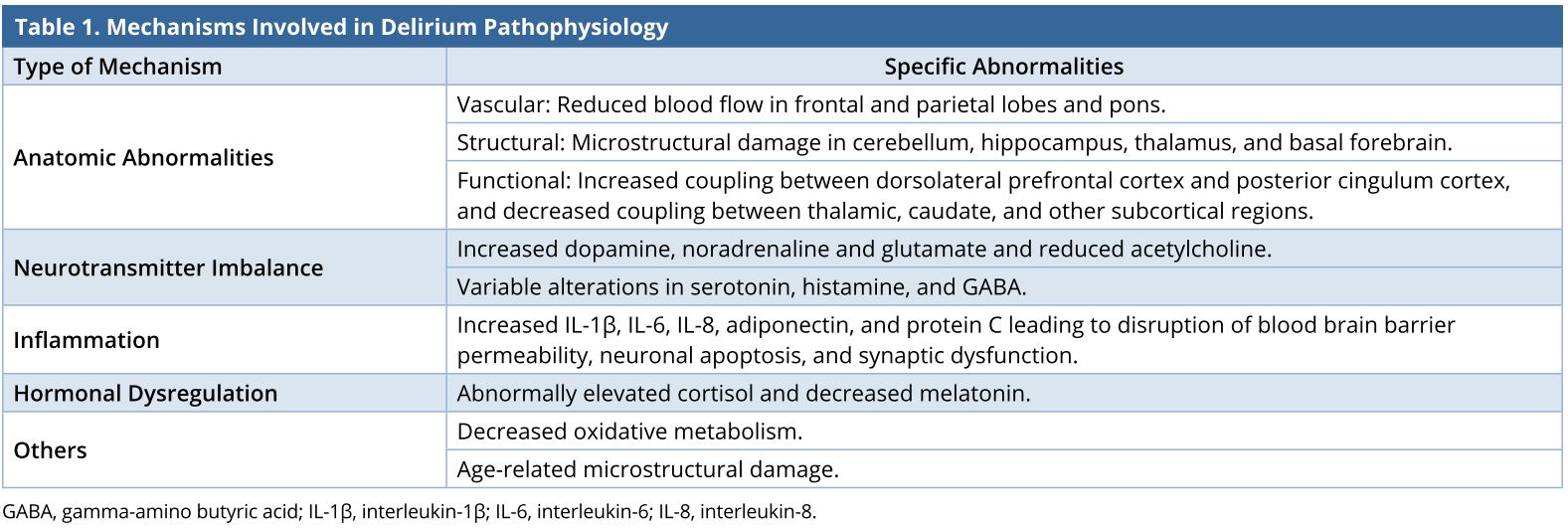
The pathophysiology of delirium is complex, multifactorial, and incompletely understood, with multiple different mechanisms contributing to the symptoms of this clinical syndrome. Several abnormalities have been described and different hypotheses developed (Table 1) to explain the changes in arousal, cognition, and perception that are the hallmarks of this disorder.
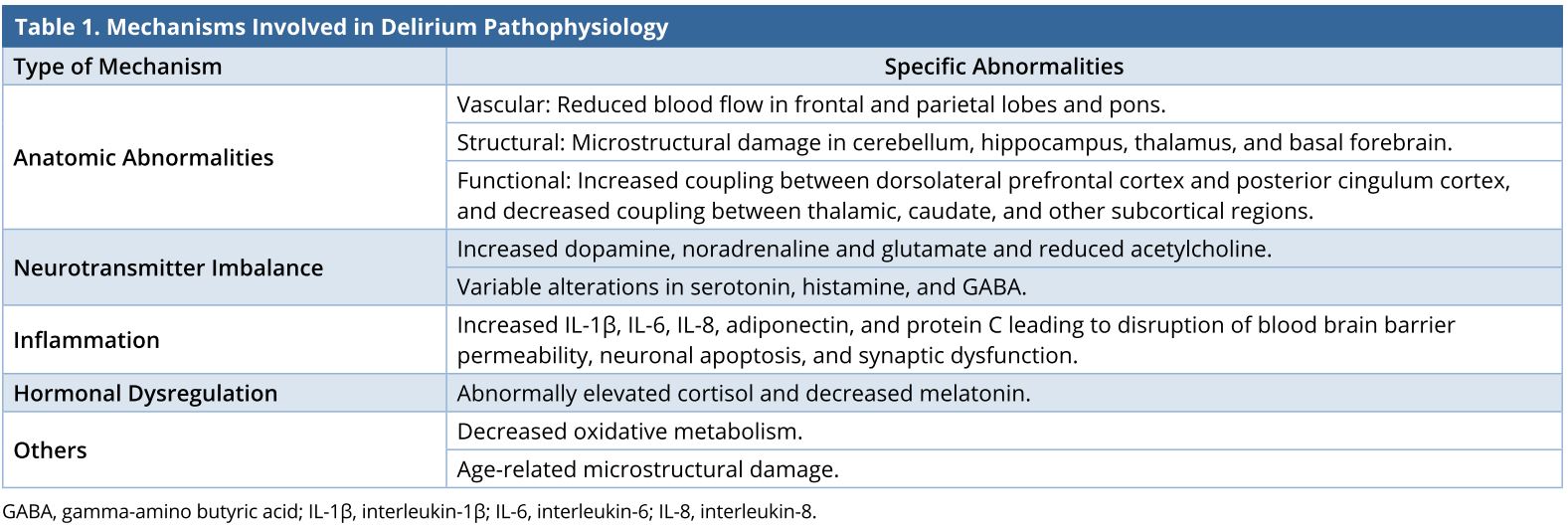
Anatomic Abnormalities
Delirium has been postulated to be caused by dysfunction in structures mediating attention, affecting the bilateral frontal lobes, primary motor cortex, right parietal lobe, thalamus and brainstem [19]. Recent neuroimaging studies have supported this idea while further elucidating localization of deficits. A study examining cerebral blood flow with single photon emission computed tomography found variable reductions in frontal, parietal and pontine regions, consistent with the role of frontal-parietal networks in attention, orientation, and cognitive control, and pontine involvement in arousal and wakefulness [20]. Another study, which examined microstructural damage in white and grey matter with diffusion tensor imaging, found abnormalities in the cerebellum, hippocampus, thalamus, and basal forebrain [21]. Clinically, these abnormalities are consistent with many of the deficits encountered in delirium, with the basal forebrain being critical in arousal, the hippocampus and temporal lobe in memory and visuospatial abilities, and the fronto-thalamic network in attention. In addition to abnormalities in specific brain structures, specific networks have also been implicated. For example, a recent study found increased resting state functional connectivity between the dorsolateral prefrontal cortex and the posterior cingulate cortex, and decreased connectivity between thalamic, caudate, and other subcortical regions [22]. Taken together, these findings highlight the multinetwork involvement of delirium with involvement of the default mode network, executive control areas, and subcortical structures. The abnormalities described likely represent accumulated structural damage and loss of connectivity that leaves patients vulnerable to delirium when exposed to increased stressors such as acute medical illness or surgery [21].
Neurotransmitter Imbalance
At the molecular level, delirium is thought to arise from a neurotransmitter imbalance leading to excess release of dopamine and reduced availability of acetylcholine [23]. This hypothesis is supported by epidemiological studies that have shown both anticholinergic medications and dopamine administration to be independent risk factors for the development of delirium [24,25]. Similarly, increases in other excitatory neurotransmitters such as glutamate and noradrenaline have been described, as well as variable alterations of gamma-amino-butyric acid (GABA), serotonin, and histamine, although evidence is conflicting or not well understood [26,27].
Inflammation
Among the best characterized risk factors in delirium is inflammation, with several interleukins (IL-1β, IL-6, IL-8), S100B (a marker of increased blood brain barrier permeability and brain damage), protein C, and adiponectin associated with its development [28-30]. Inflammation is suspected to cause disruptions in the blood brain barrier and infiltration of leukocytes and cytokines, leading to neuronal apoptosis and synaptic dysfunction [31].
Hormonal Dysregulation
Circadian dysregulation leading to alterations in normal sleep architecture and disturbances in the hypothalamic-pituitary-adrenal axis leading to abnormally elevated levels of cortisol may also play a role [32]. Abnormally low levels of serum melatonin have been observed in ICU patients with delirium [33], and different delirium subtypes have been associated with either increased or decreased urinary melatonin metabolites [34]. Studies have shown that both pre- and postoperative elevated levels of cortisol correlate with delirium [35,36], and failure to suppress secretion after dexamethasone administration has been correlated with risk of delirium in patients with stroke and dementia [37,38]. Elevated levels of glucocorticoids are postulated to leave neurons vulnerable to additional stressors [39].
Other Mechanisms
Associated factors include decreased oxidative metabolism secondary to atherosclerosis and ischemia [40], although studies examining the relation of white matter hyperintensities to delirium have produced conflicting results [41,42]. Finally, changes in the microarchitecture of the brain secondary to aging, with gradual accumulation of damage to neurons and astrocytes have also been postulated [43,44].
Causes of delirium may be grouped into either predisposing factors (vulnerabilities) or precipitating factors (triggers) [45]. Some of the most common predisposing factors include older age, dementia, multiple medical illnesses, history of alcohol use, sensory impairments, depression, and poor functional status [46], while common precipitants in hospitalized patients include medications (particularly psychotropic medications), infection, metabolic abnormalities, surgery, urinary catheterization, and pain [47,48]. Predisposing factors are of clinical importance in identifying patients at high risk of delirium in hospital settings [46], since a greater burden of predisposing factors renders patients more at risk for developing delirium in the presence of fewer precipitating factors. Models to predict delirium, such as the PRE-DELIRIC (Prediction of Delirium in ICU Patients) have been developed with promising results [49], but it is not yet clear that these models offer a reliable predictive value in older patient populations, who may benefit most from screening.
Delirium should be treated as a medical emergency until proven otherwise, with many potentially fatal etiologies—including seizures, intracranial bleeding, hypoxemia, hypoglycemia, hypertensive crisis, infection, metabolic or electrolyte abnormalities, and substance intoxication or withdrawal—ruled out early in its presentation. “Hospital delirium” or “ICU delirium” does not exist, and delirium should never be attributed to the mere environment of the hospital setting.
Delirious patients may present as agitated or stuporous, with paranoia, frank delusions, visual hallucinations, disorganized thinking, and disorientation; subtypes of delirium include hyperactive, hypoactive, or mixed [50]. A key component of delirium is its fluctuating nature, often described as waxing and waning: patients may appear alternately lucid and disoriented. The DSM-5 and ICD-10 diagnostic criteria differ slightly but both reflect this general definition [1,2].
Prompt identification of delirium is critical, as delirium may be the sole manifestation of systemic illness, and correct identification will lead to investigation of the underlying pathology. Of the numerous formal measures available, the Confusion Assessment Method (CAM) is the most widely used [51] and has been adapted for specific environments requiring more rapid assessments [52], such as intensive care settings [8]. Additional diagnostic measures, such as the 4AT test, have also demonstrated similar sensitivities and specificities [53], and the latter may be more reliable in diagnosing the hypoactive subtype [54]. More recently, so-called “ultrabrief” measures (such as asking the patient to recite the months of the year backward) have also demonstrated high sensitivity [55], although the generalizability of these briefer screens needs further study [56].
Importantly, most validation studies of delirium assessment tools were performed by researchers who were specifically trained in the measure being studied, which may limit generalizability [54]. When evaluating for possible delirium in inpatient settings, it is useful to include both a structured examination of the patient that includes screening for inattention, disorientation, changes in arousal, and bizarre thought content, along with observation of any abnormalities in grooming, dress, affect, speech, or motoric changes. Since an integral element of delirium is its fluctuating nature, it is essential to gather information regarding the patient’s mental state over time, closely review prior documentation for clues of changes in mental state, and review objective information (e.g., labs, culture data, imaging) for evidence of common precipitating causes of delirium. In cases where the patient’s baseline may be unclear, collateral information from a family member can provide additional useful information.
Non-pharmacologic guidelines for the prevention of delirium in hospitalized patients have been developed and implemented with successful reduction in incidence and associated functional decline [57]; these guidelines have also been adapted for use in the perioperative setting [58], and a recent meta-analysis of 14 studies found significant reductions in incidence of both delirium and falls [59]. These multi-component strategies target physical, cognitive, functional, and sensory parameters and include interventions such as frequent reorientation, early mobilization, sleep cycle regulation, and correction of hearing and visual deficits.
Pharmacologic interventions have also been investigated for the prevention of delirium; however, these interventions have yielded mixed results. Despite promising studies finding that antipsychotics were effective in reducing either the incidence [60] or the severity of post-operative delirium following elective major surgery [61], trials in critical care populations have not found benefit in reducing delirium incidence [62] or survival [63]. Larger meta-analyses of hospitalized patients have not found evidence supporting the use of antipsychotics as a preventative strategy [64,65]. Recent meta-analyses regarding melatonin or melatonin receptor agonist prophylaxis have reached conflicting conclusions; whereas a Cochrane review did not find evidence that melatonin treatment prevented delirium [65], a meta-analysis published the same year found that patients admitted for medical, but not surgical conditions benefited from melatonin or ramelteon [66]. Dexmedetomidine has generated interest following promising studies across various ICU patient populations, the results of which appear to be supported by a meta-analysis of 14 randomized trials including over 3,000 medical and surgical ICU patients, which found that dexmedetomidine administration resulted in a significantly decreased incidence of delirium [67].
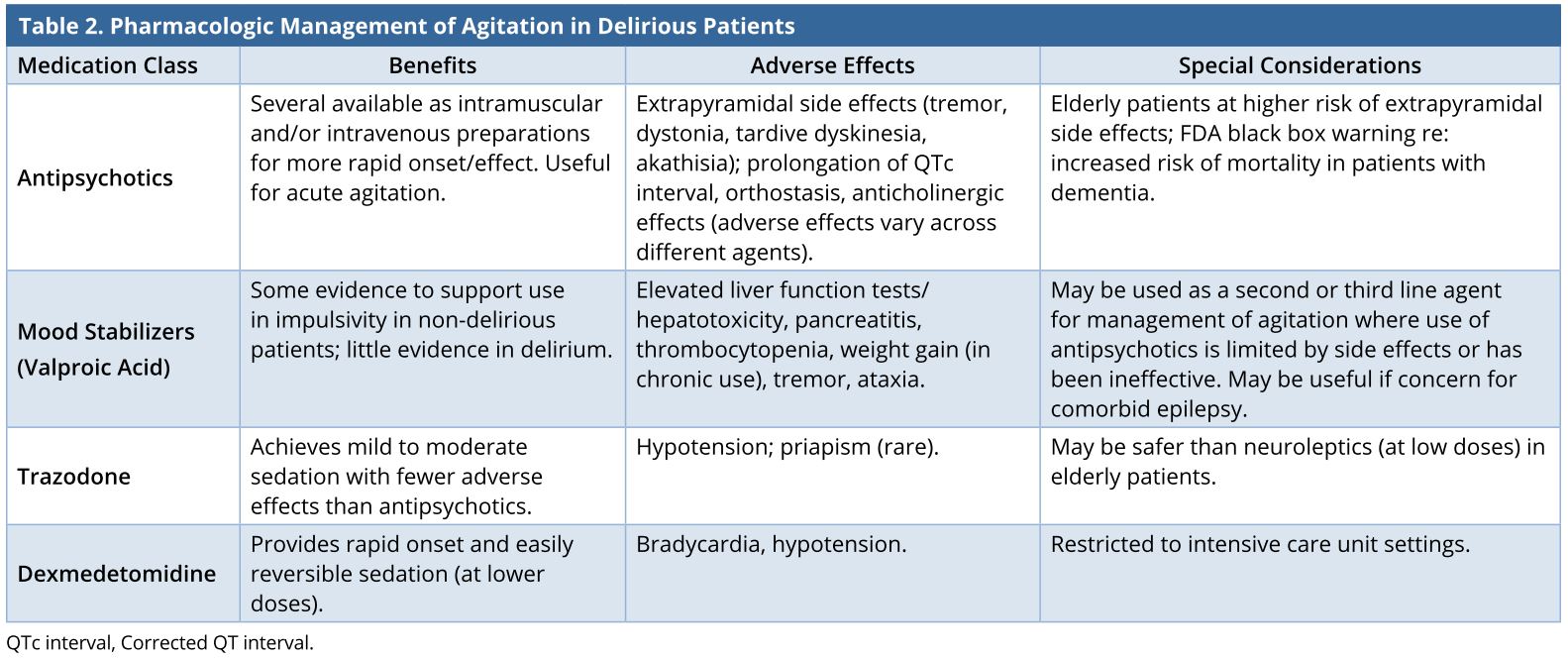
The main strategy for managing delirium is to identify and reverse its underlying causes; this is especially important when the cause has the potential to be serious or life-threatening. However, despite adequate treatment, it may take substantial time before delirium resolves, especially for patients who have multiple underlying risk factors for delirium. When delirium is accompanied by significant agitation that interferes with care (e.g., pulling at catheters or central lines), pharmacologic interventions frequently are employed to improve patient safety and comfort (Table 2).
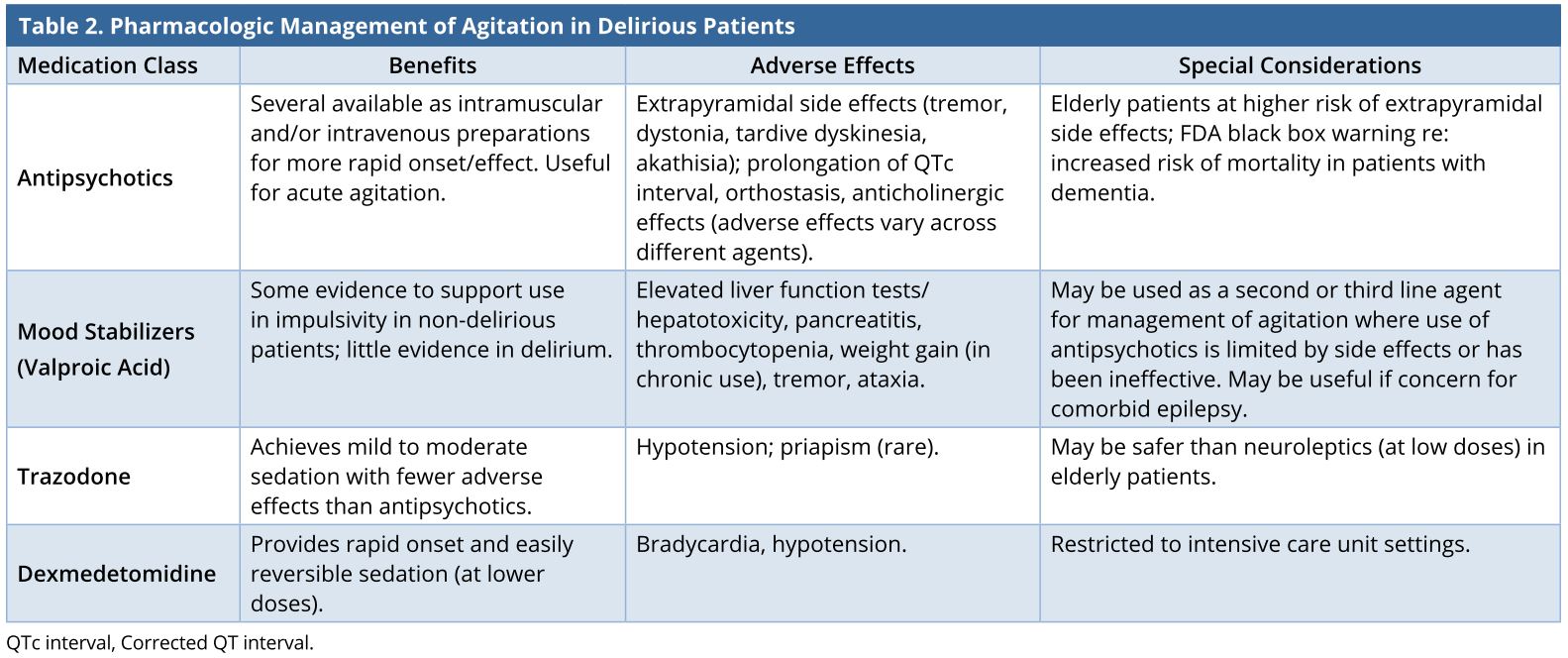
Antipsychotics
Antipsychotic medications have long been considered mainstays of treatment for agitation in delirium. Of these agents, haloperidol remains the oldest and best-studied, although most studies are small, unblinded, and limited to delirium in specific settings or disease states. A Cochrane review and meta-analysis examining antipsychotics for delirium included three studies where haloperidol was compared to olanzapine, risperidone, or placebo, respectively, and found no difference in delirium scores between groups treated with haloperidol or atypical antipsychotics; however, haloperidol was more effective than placebo [68]. Neither individual studies nor pooled data have found significant differences in efficacy between specific antipsychotic agents, or between-group differences comparing typical agents to the newer atypical antipsychotics such as olanzapine [69], risperidone [70], or aripiprazole [71,72].
More recent literature has called into question the efficacy of antipsychotics in reducing the severity of symptoms or duration of delirium due to severe methodological limitations of studies, including lack of adequate control groups, small sample size, non-randomization, or absence of placebo [73]. Furthermore, a recent Cochrane review specifically examining non-ICU patients did not find evidence that antipsychotics (typical or atypical) reduced severity or resolved symptoms of delirium [74]. They also noted the lack of observation across all studies of longer term delirium outcomes such as hospital length of stay, long-term health-related quality of life, or cognitive outcomes [74]. Additionally, antipsychotics are associated with a risk of several adverse effects, such as prolongation of the corrected QT interval and risk of torsades de pointes [75,76]. Patients at the greatest risk for delirium also appear to be at highest risk of several antipsychotic-related adverse effects, with the risk of tardive dyskinesia being three to five times greater in patients over the age of 55 [77]. Of greater concern, in 2003 the Food and Drug Administration warned prescribers of an increased risk of cerebrovascular events in elderly patients being given atypical antipsychotics [78], and in 2005, issued a black-box warning about increased all-cause mortality in elderly patients with dementia taking atypical antipsychotics [79]. Though these findings have proven somewhat controversial, caution should be exercised when using these agents in delirium, particularly in elderly patients with dementia.
Anticonvulsants, Anxiolytics, and Antidepressants
Due to its limited effect on the corrected QT interval, action on multiple neurotransmitter systems, and use in agitation secondary to other disorders, such as traumatic brain injury [80], valproic acid has been proposed as an alternative to antipsychotics in the management of clinical symptoms of hyperactive and mixed delirium, particularly in cases where conventional therapy is inadequate or limited [81]. However, studies supporting its efficacy are limited to small case series and one retrospective study, which found improvement in delirium symptoms following treatment [82]. To the authors’ knowledge, other anticonvulsants, such as carbamazepine and gabapentin, have not been studied for treating delirium. There is not currently evidence to support the use of benzodiazepines in the treatment of delirium not associated with alcohol or GABA agonist withdrawal syndromes [83], but they may sometimes be used as an adjunct with haloperidol, both for reduction in severe agitation as well in prevention of extrapyramidal symptoms [84]. Of the antidepressants, trazodone has been used due to its sedative properties, but with little evidence supporting its use [85].
Alpha-2 Adrenergic Agonists
Alpha-2 adrenergic agonists are centrally acting compounds that reduce noradrenergic activity and induce sedation; they are particularly attractive for managing agitation in hospital settings due to their absence of effect on respiratory drive [86]. Initially used as a centrally-acting antihypertensive agent, clonidine is sometimes used for sedation in intensive care settings, despite a lack of clinical trials supporting its use, which is frequently limited by clinically significant hypotension [87]. Dexmedetomidine, which is 7-8 times more selective than clonidine for alpha-2 versus alpha-1 receptors, has fewer adverse effects than clonidine on heart rate and blood pressure [88]; these remain common, however, and use of dexmedetomidine is currently limited to intensive care settings. As the risk of bradycardia and hypotension may be at least partially related to whether or not a loading dose is administered, specific dosing protocols may be used to minimize the risk of hypotension [89]. Dexmedetomidine has been increasingly investigated as a treatment for delirium in the intensive-care setting, with a randomized but open-label trial finding superiority over haloperidol in treating delirious, intubated patients [90], and a recent, randomized and placebo-controlled trial finding an increase in ventilator-free hours in intubated patients with agitated delirium limiting extubation [91].
In practice, based on the available evidence as well as clinical experience, antipsychotics will likely remain the standard of care for the foreseeable future for the management of acute agitation secondary to delirium in cases where behavioral interventions have failed. For agitation secondary to delirium in the intensive care unit, particularly for ventilated patients, dexmedetomidine may be a reasonable alternative. In cases that are refractory to these agents or when treatment is limited by intolerable or unsafe adverse effects, mood stabilizers may be considered as an alternative.
Delirium is a commonly encountered clinical entity that is associated with poor cognitive and physical health outcomes. Although its pathophysiology remains poorly understood, both structural and molecular factors may contribute to its clinical symptoms. Given its impact on health, programs to identify those at risk for delirium, prevent the incidence of delirium, and identify it early are critically important. If delirium is diagnosed, treatment remains identifying and addressing its underlying cause. While some evidence indicates that pharmacologic agents may be beneficial in specific patient populations, evidence for use is limited, and, in the absence of acute agitation, the widespread use of medications across all delirium patient populations should be discouraged. Future research should focus on better understanding the pathophysiology, identification, and treatment of delirium, as minimizing its incidence and duration has the potential to improve both mental and physical health in the short- and long-term.
Received date: September 18, 2018
Accepted date: September 28, 2018
Published date: October 12, 2018
None
None
© 2018 The Author (s). This is an open-access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC-BY).
ICG lymphography is an invaluable tool in lymphedema management. Both immediate and delayed scans are needed when performing the study. The delayed scan needs to be performed at the time of the lymphographic plateau to appreciate the full extent of the pathology. Using a recumbent cross trainer, the lymphographic plateau can be achieved in 15 minutes following ICG injection. We have found this exercise enhanced ICG lymphography protocol worthwhile of adoption by high volume lymphedema centers to raise diagnostic accuracy and efficiency.
This article presents a comprehensive review of schwannomatosis affecting cranial nerves, delineating its unique characteristics distinct from other forms of neurofibromatosis. By addressing diagnostic complexities and the evolving criteria for identification, the paper emphasizes the critical need for accurate recognition of schwannomatosis to facilitate effective management and provide essential genetic counseling. Enriched with a detailed case study, this review delivers vital insights into the epidemiology, symptomatology, and therapeutic strategies for schwannomatosis, advocating for a revision in current clinical approaches. This work is indispensable for medical professionals aiming to enhance diagnostic precision, comprehend genetic underpinnings, and improve patient outcomes. Offering a thorough analysis of this rare condition, the article is pivotal not only for clinicians and researchers in the neurogenetic field but also for a broader spectrum of medical and scientific communities, bridging a notable gap in contemporary medical literature.
The article stands out by providing a comprehensive analysis of a rare case of a midline branchial cleft cyst, a significant contribution given that only three other cases have been documented in medical literature. This scarcity underscores the article's value, making it a crucial read for medical professionals. It not only highlights the diagnostic challenges and treatment strategies for such atypical presentations but also enriches the understanding of branchial cleft cysts beyond the common lateral neck occurrences. By including a detailed review and comparative analysis of these few reported cases, the article offers unique insights into the demographic, symptomatic, and anatomical variations of branchial cleft cysts. This focused analysis makes the article an indispensable resource for clinicians, surgeons, and students in the medical field, aiming to enhance diagnostic accuracy, inform clinical practice, and ultimately improve patient outcomes in dealing with complex and rare presentations of congenital anomalies.
AI is rapidly evolving from a supportive tool into a core component of medical decision making and evidence synthesis, reshaping how clinicians interpret information at the point of care. Yet, while much of medical AI research emphasizes algorithmic performance and explainability, it seldom addresses the more practical question: how should physicians evaluate an AI recommendation in real-world, high-risk situations when fluent outputs can conceal critical errors. This Perspective offers a clinician-centered framework that treats AI outputs as provisional, testable hypotheses rather than definitive conclusions. By guiding users through premise verification, terminological precision, evidence appraisal, and causal analysis, it provides a structured defense against hallucinations, selective reporting, and data poisoning, using otolaryngology as a high-stakes, multimodal model. By placing clinical judgment at the center of AI use, this work shifts the field from passive automation toward safer, more accountable decision support grounded in patient safety.
A paradigm shift in type 2 diabetes may contribute to the reinforcement of new research questions and further improvement of diabetes care in clinical practice.
The PLOSEA technique detailed in this study addresses the significant challenge of managing large vessel size discrepancies in microvascular surgery with an innovative and accessible method. By partially obliterating the larger vessel lumen before anastomosis, the technique reduces risks of thrombosis and misalignment, simplifying the procedure without sacrificing effectiveness. This advancement is particularly valuable as it allows surgeons with varying levels of experience to perform complex reconstructions with greater confidence and improved patient outcomes. A key feature is the inclusion of a detailed video demonstration, providing a dynamic and comprehensive visual guide that surpasses traditional static images. This video meticulously elucidates each procedural step, enhancing understanding and facilitating the practical application of the technique. Emphasizing technical precision, patient safety, and surgical efficiency, this study offers a compelling narrative for medical professionals. The transformative impact of the PLOSEA technique on surgical practice underscores its importance, presenting a novel approach that can enhance the quality of care and expand the capabilities of microsurgeons worldwide.
This study investigates the efficacy of conservative management using 5-fluorouracil (5-FU) for treating cholesteatoma in ambulatory care settings, offering an alternative for patients who prefer to avoid surgery. Over 13 years, 15 ears of 14 patients were treated with a 5% 5-FU cream and assessed using Takahashi's efficacy criteria. The results revealed positive outcomes, with 87% of cases deemed good and 13% as fair, with no poor evaluations. This approach may be suitable for specific populations, such as older adults and individuals in remote areas with limited access to specialized healthcare services.
This article presents a comprehensive review of schwannomatosis affecting cranial nerves, delineating its unique characteristics distinct from other forms of neurofibromatosis. By addressing diagnostic complexities and the evolving criteria for identification, the paper emphasizes the critical need for accurate recognition of schwannomatosis to facilitate effective management and provide essential genetic counseling. Enriched with a detailed case study, this review delivers vital insights into the epidemiology, symptomatology, and therapeutic strategies for schwannomatosis, advocating for a revision in current clinical approaches. This work is indispensable for medical professionals aiming to enhance diagnostic precision, comprehend genetic underpinnings, and improve patient outcomes. Offering a thorough analysis of this rare condition, the article is pivotal not only for clinicians and researchers in the neurogenetic field but also for a broader spectrum of medical and scientific communities, bridging a notable gap in contemporary medical literature.
This article presents a comprehensive discussion of advanced techniques in managing pediatric airway obstructions caused by vallecular cysts. By employing awake fiberoptic intubation and transoral CO₂ laser microsurgery, the authors highlight a thoughtful, evidence-based approach that emphasizes both safety and precision. While not groundbreaking, the depth of analysis in the decision-making process and procedural techniques offers invaluable insights for clinicians, particularly in pediatric otolaryngology. The article serves as a critical reference for handling complex airway cases, balancing innovative practices with established methods. Its significance lies in its contribution to optimizing patient safety, particularly in high-risk infant cases, making it essential reading for healthcare providers dealing with airway management challenges.
Motorcycle chain-induced fingertip amputations represent a reconstructive dead end, where severe crushing and contamination traditionally compel revision amputation. The authors dismantle this exclusion criterion, reporting an 83% salvage rate using a modified protocol of radical debridement, strategic skeletal shortening, and simplified single-vessel supermicrosurgery. By eschewing complex grafting for tension-free primary anastomosis, the authors successfully restored perfusion in ostensibly
This is an excellent article that comprehensively reviews and updates the topic on delirium regarding its epidemiology, pathophysiology, diagnosis, prevention, and management. I believe this paper will be of interest to readers and deserves the widest attention. I recommend its publication in the current form.
Ospina JP, King IV F, Madva E, Celano CM. Epidemiology, mechanisms, diagnosis, and treatment of delirium: A narrative review. Clin Med Ther 2018;1(1):3. https://doi.org/10.24983/scitemed.cmt.2018.00085
 PDF
PDF